Central Venous Line
Placement.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
- Central access is the backbone of neuro-ICU care — pressors, monitoring, dialysis, TPN.
- Baseline CLABSI rates of 0.8–2.0 per 1,000 catheter-days are achievable only with rigorous bundle adherence.
- Subclavian pneumothorax rate is 0.5–5% even with experienced operators.
- CMS classifies a retained guidewire as a Never Event — zero tolerance, mandatory reporting.
Takeshita J et al. BMC Infect Dis. 2022;22(1):772 · PMID 36195853
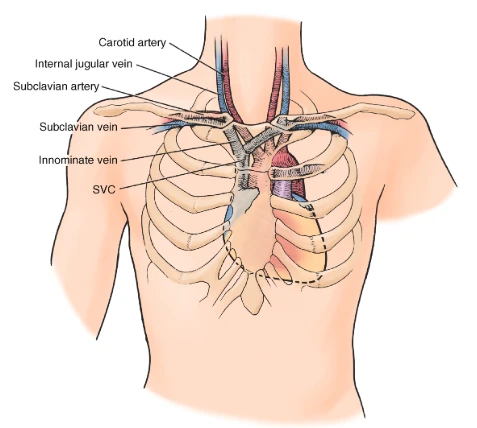
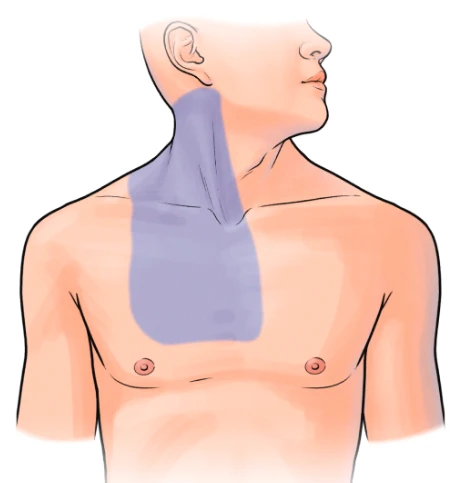
Anatomy & site selection.
Describe vascular anatomy at IJ, SC, and femoral; differentiate sites by infection, mechanical, and DVT risk.
Ultrasound-guided access.
Perform US pre-scan, vein-vs-artery discrimination, dynamic needle-tip tracking under real-time guidance.
Seldinger mastery.
Execute puncture, wire, confirmation, dilation, catheter — with wire-never-lost control through every step.
Complication recognition.
Recognize immediate and delayed events; escalate arterial dilation, pneumothorax, retained wire appropriately.
Bundle adherence.
Execute the CDC / AHRQ insertion bundle: maximal barrier, CHG antisepsis, site selection, daily review.
Confirmation & documentation.
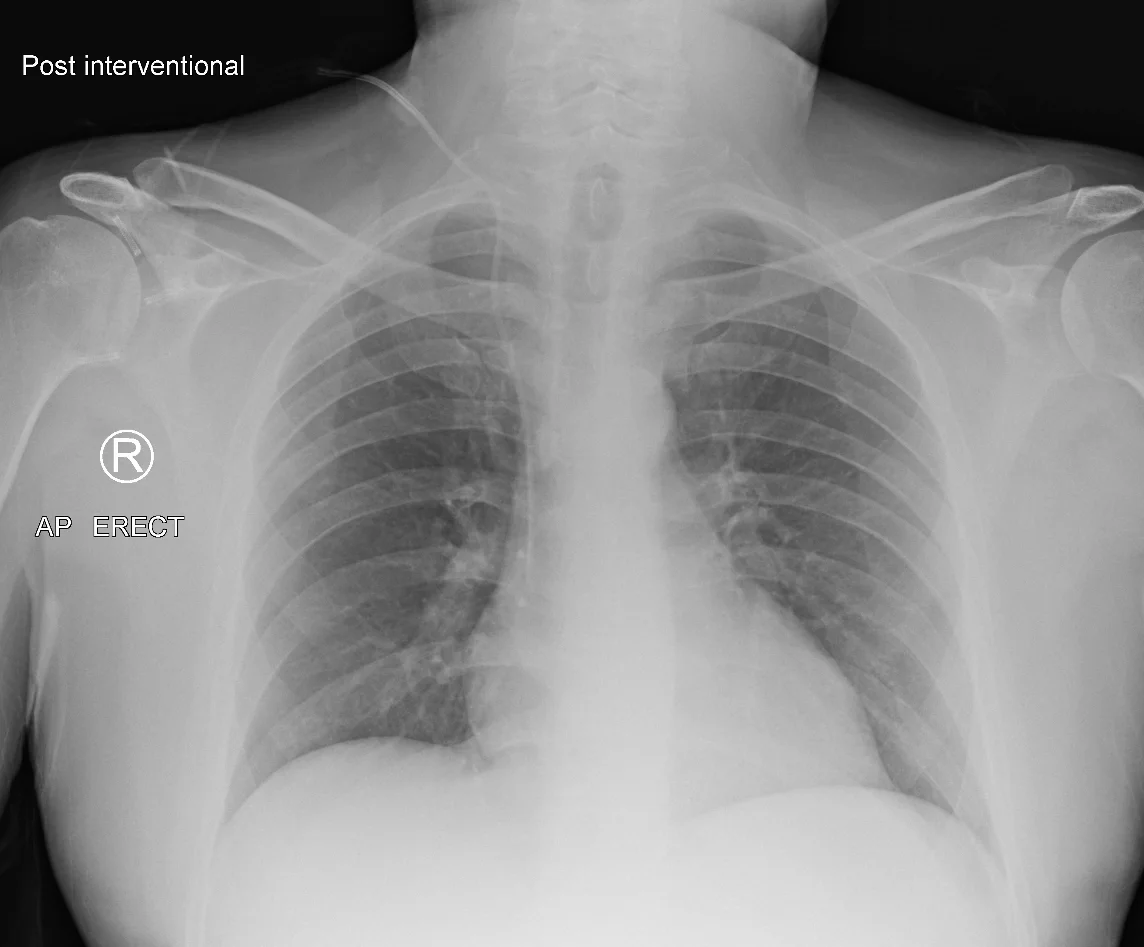
Confirm tip at SVC/RA on CXR; document fully; lead a TJC-compliant time-out before every case.
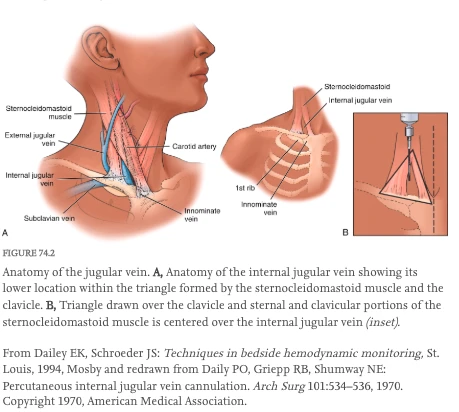
Anatomy & site selection.
Dailey & Schroeder 1994 (Mosby) · redrawn from Daily, Griepp & Shumway, Arch Surg 1970 · educational fair use
The straight path
to the SVC.
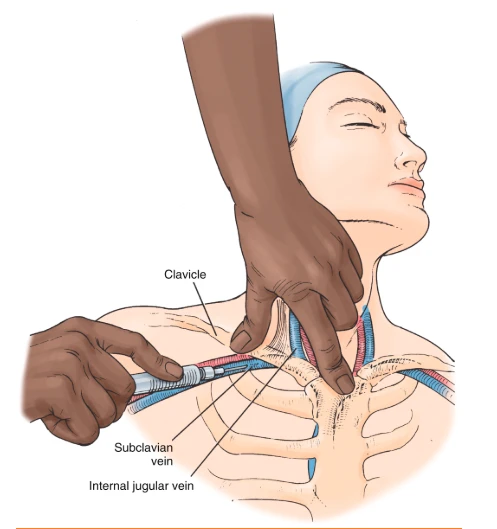
- Lateral & anterior to carotid · compressible, non-pulsatile on US
- Trendelenburg + slight contralateral head turn
- Lowest mechanical risk under US guidance
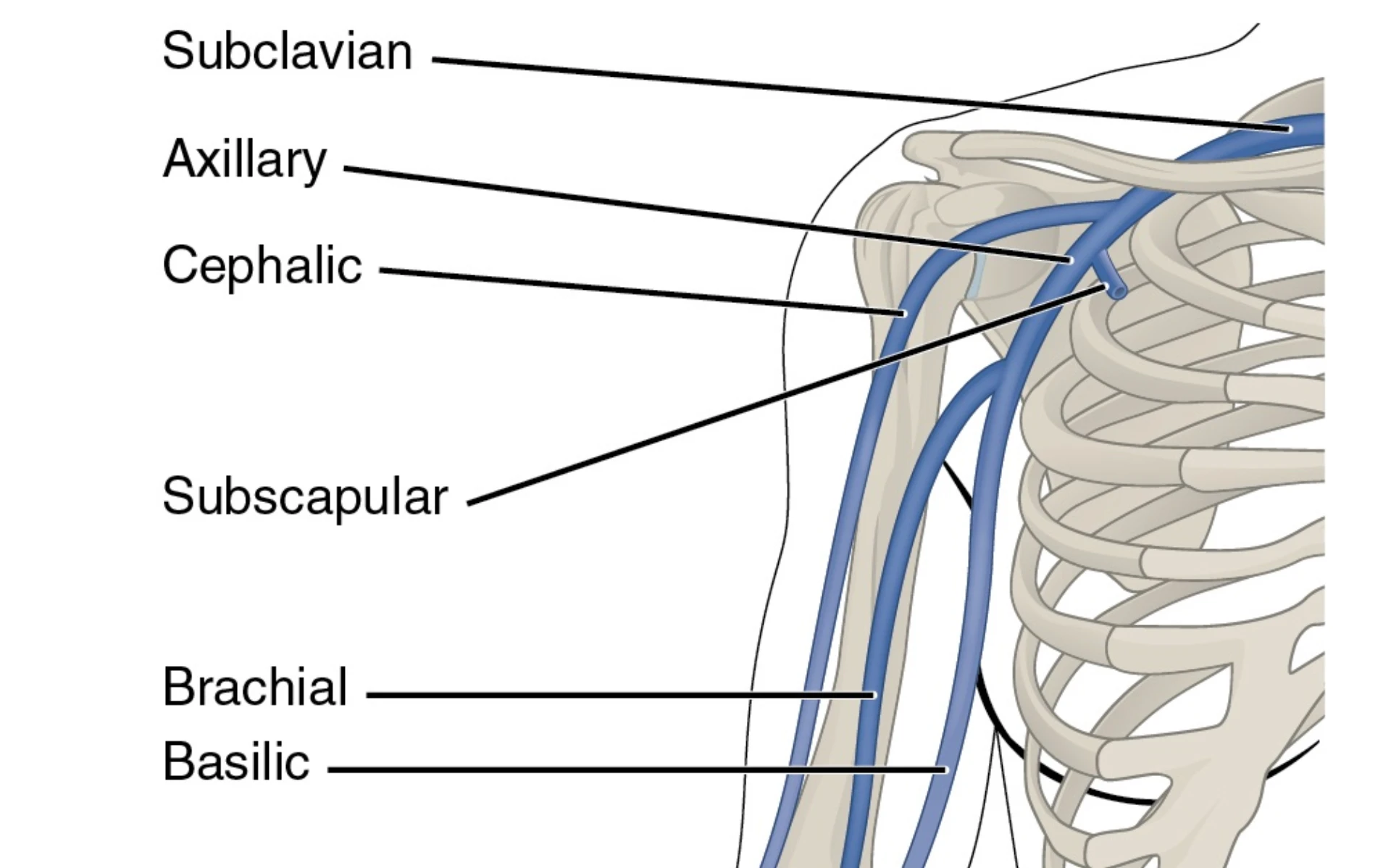
Lowest infection,
highest pneumothorax.
- Pleural dome lies immediately inferior & posterior
- Pneumothorax rate 0.5–5% with experienced hands
- Avoid in coagulopathic patients — non-compressible

No lung at risk —
review at 72 h.
- Vein medial & deep to femoral artery (NAVEL)
- Highest historical DVT risk for long dwell
- Preferred for emergency / code access
| Clinical context | IJ | Subclavian | Femoral | Why |
|---|---|---|---|---|
| Stable neuro-ICU workhorse | Preferred | Acceptable | Avoid | US-guided IJ has lowest combined complication rate in NCC populations. |
| Coagulopathy / on anticoag | OK | Avoid | OK | Subclavian is non-compressible; IJ and femoral are compressible if bleeding. |
| Emergency / code access | OK | Avoid | Preferred | Fastest access, no airway competition, zero pneumothorax risk. |
| Long-term dwell (> 7 days) | Acceptable | Preferred | Avoid | CDC 2011: lowest infection rate at subclavian for prolonged dwell. |
| Contralateral pneumothorax | OK | Absolute contra | OK | Bilateral pneumothorax converts a complication into a code. |
- Vasopressor / inotrope administration
- Hemodynamic monitoring (CVP, ScvO2)
- Hemodialysis access
- Total parenteral nutrition (TPN)
- Poor peripheral access in critically ill patient
- Rapid volume resuscitation — Cordis or large-bore PIV outperforms triple-lumen CVC
- Absolute: infection at insertion site
- Absolute for SC: uncorrected coagulopathy · contralateral pneumothorax
- Absolute: ipsilateral venous thrombus · distorted anatomy
- PLT < 20k urgent / < 50k elective — 1U platelets pre-procedure as needed
- INR > 1.8 urgent / > 1.4 elective
- 01Consent documented. Indication, risks, alternatives, right to decline — teach-back confirmed. Surrogate decision-maker engaged if patient lacks capacity.
- 02Labs reviewed. PLT ≥ 50k urgent / ≥ 100k elective · INR ≤ 1.8 urgent / ≤ 1.4 elective. Imaging reviewed (prior CXR, relevant CT).
- 03Site decision made. Communicated to team — bedside RN and any assistant know the plan and the why.
- 04Patient positioned. IJ — Trendelenburg, contralateral head turn. SC — Trendelenburg + shoulder roll. Fem — supine, slight reverse-T, leg abducted.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, site / side, equipment, consent confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
hygiene.
barrier.
prep.
selection.
review.
- CHG-alcohol prep (2% CHG / 70% IPA)
- Cap, mask, sterile gown, gloves
- Large full-body fenestrated drape
- Sterile probe sleeve + sterile gel
- 1% lidocaine + 25g needle
- Finder needle (22g) · introducer 18g
- 0.035-inch J-tip guidewire
- #11 scalpel blade
- Tissue dilator
- Triple-lumen catheter (7 Fr UCI standard)
- Sterile pressure transducer tubing
- 3-0 suture · CHG occlusive dressing
- Linear high-frequency probe (10–12 MHz)
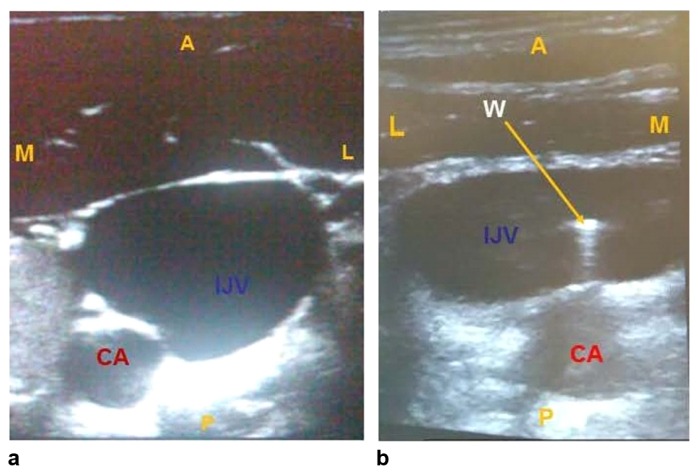
- Short-axis confirms compressibility (vein) vs pulsatility (artery)
- IJ lies lateral to carotid, compressible, non-pulsatile
- Map vessel — note depth, diameter, any thrombus
- Identify variants (small IJ, overlapping vessels)
- Mark skin entry with probe footprint
The Seldinger
sequence.

Dctrzl · Wikimedia · CC BY-SA 4.0
Skin prep ·
maximal barrier.
- CHG-alcohol, concentric circles, center out
- ≥ 30 s dry time — do not blot, do not fan
- Full barrier: cap, mask, gown, gloves, drape
- Sterile probe sleeve + sterile gel
Probe orientation ·
needle trajectory.
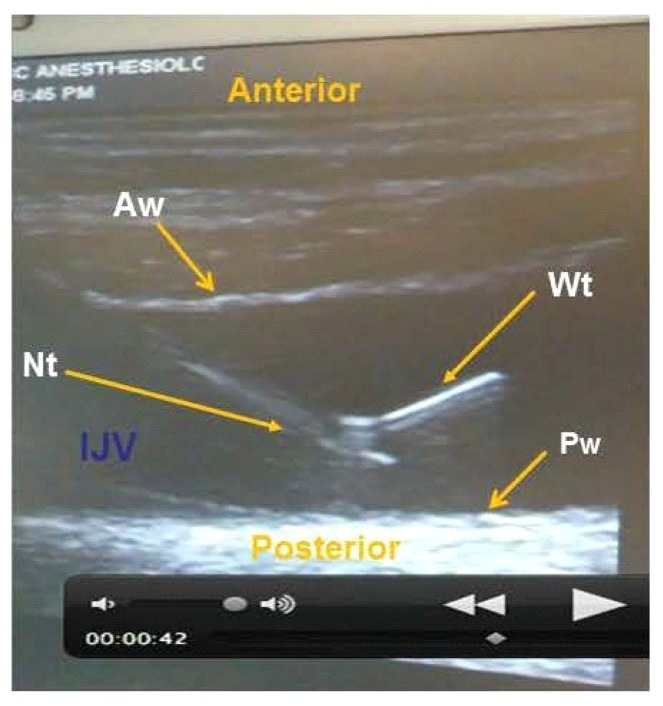
- Short-axis (out-of-plane): bee-sting tip view
- Long-axis (in-plane): full shaft visible
- IJ — ~45° angle, 1 cm above probe edge
- SC — 10–15° posterior to clavicle midpoint
- Fem — ~45°, short-axis over vein
Venous puncture ·
dark, non-pulsatile.
- Dynamic tip tracking, small increments
- Aspirate on advance — flash of dark blood
- Disconnect syringe: blood drips, doesn't spurt
- Pulsatile / bright red — withdraw, hold pressure
Confirm wire in vein
before you dilate.
Wire appears as a bright echogenic line inside the vein. Sweep short-axis, confirm artery is clean.
Sterile tubing on wire shows a venous waveform — low pressure, respiratory variation — not a pulsatile arterial trace.
Consult vascular surgery.
Takeshita J et al. BMC Infect Dis. 2022;22(1):772
Wire ·
tip-first.
- J-tip first — vessel-friendly
- Monitor ECG · PVC → wire too deep
- Pull back 2–3 cm if ectopy
- WIRE-NEVER-LOST · one hand always.
Skin nick ·
parallel to wire.
- #11 blade, superficial only
- Blade parallel to wire, never across
- Just enough to pass dilator
Dilator ·
fascia only.
- Gentle twist over wire
- Never advance to the hub — back-wall injury
- Opens fascia · does not enter vessel
- Withdraw dilator, wire stays seated
Catheter ·
depth by site.
- Right IJ ≈ 15 cm · Left IJ ≈ 17 cm
- Subclavian ≈ 15 cm · Femoral ≈ 20 cm
- Peres 1990: right IJ ≈ heightcm/10
- Wire exits brown port before final seating
- Withdraw wire in one smooth motion · do not re-advance
- Cap each lumen immediately after wire removal
- Aspirate each port: dark blood return on all lumens
- Flush each with 10 mL NS · clamp unused lumens
- Confirm no air aspirated or flushed
- 3-0 non-absorbable suture at wing clamps · two-point fixation
- CHG-impregnated transparent occlusive dressing (BioPatch)
- Document depth marker (cm at skin) on chart
- Date and initial the dressing per nursing protocol
Arterial puncture.
Bright pulsatile blood. Withdraw, hold pressure 10–15 min. If dilated — emergent vascular surgery.
Pneumothorax.
SC > IJ > Fem (zero). Post-CXR diagnosis. Chest tube if symptomatic; observe small apical.
Arrhythmia.
PVCs / atrial ectopy from deep wire. Pull wire back 2–3 cm. Self-resolves if recognized early.
Air embolism.
Cap lumens promptly. Trendelenburg + left lateral decubitus if suspected. Prevention > treatment.
CLABSI.
0.8–2.0 / 1,000 catheter-days baseline. Bundle adherence is primary prevention. NHSN-reportable.
Catheter-related DVT.
Highest with femoral. Daily review for line necessity. Remove as soon as clinically feasible.
Catheter malposition.
Tip in contralateral brachiocephalic or azygos. Diagnosed on CXR. Reposition or replace.
Retained guidewire.
CMS Never Event. 100% preventable with wire-never-lost principle. IR retrieval if it occurs.
Dilating without wire-in-vein confirmation.
The single most dangerous error in this procedure. Always confirm position by US re-scan or pressure transduction before dilation.
Losing the wire.
A retained guidewire is a CMS Never Event. One hand on the wire from insertion through final catheter seating.
Skipping Trendelenburg for IJ / SC.
Flat positioning reduces venous distension and raises air-embolism risk. Always Trendelenburg for IJ and SC access.
Femoral lines · no 72-hour review.
Review at 72 h is mandatory; routine removal is not evidence-based. Pull only on infection or DVT signs — but pull early when you see them.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of CVL privilege | First 5 independent cases · ≥1 each IJ / SC / Fem · within 6 months |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication or CLABSI |
| Reinstatement | < 6 cases over 24 mo | 2 proctored cases · directly observed bundle adherence |
| Renewal | Biennial · 22 CCR §70703 (CA) | OPPE indicators aggregate · Chair sign-off |
- Successful placement ≥ 95%
- US used for every IJ attempt 100%
- Wire-in-vein confirmation documented 100%
- CLABSI rate ≤ institutional target
- Post-procedure CXR before use (IJ/SC) 100%
- Daily line-necessity review documented 100%
- 01O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162–e193. PMID 21460264.
- 02Takeshita J, Tachibana K, Nakajima Y, Shime N. Incidence of catheter-related bloodstream infections following ultrasound-guided central venous catheterization: a systematic review and meta-analysis. BMC Infect Dis. 2022;22(1):772. PMID 36195853.
- 03Zawadka M, La Via L, Wong A, et al. Real-time ultrasound guidance as compared with landmark technique for subclavian central venous cannulation: a systematic review and meta-analysis with trial sequential analysis. Crit Care Med. 2023;51(5):642–652. PMID 36861982.
- 04Pronovost P, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725–32. PMID 17192537.
- 05AHRQ. CLABSI toolkit. AHRQ Safety Program for Intensive Care Units. Rockville, MD; 2020.
- 06The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 06aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 06bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 06cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 06dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 06eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 06fThe Joint Commission. NPSG.06.01.01 — clinical alarm safety; clinically appropriate settings, authority to change parameters, monitoring/response, and periodic accuracy checks for high-risk alarms. National Patient Safety Goals (HAP); effective January 2025.
- 07The Joint Commission. IC.02.02.01 — implement evidence-based practices to prevent HAIs (isolation precautions, PPE, transmission-based controls; hand-hygiene anchor is now NPSG.07.01.01 below). 2024.
- 08CDC HICPAC. Guidelines for the prevention of intravascular catheter-related infections, 2011. Atlanta, GA; 2011.
- 09Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2024;47(1S):S1–S285.
- 10Buetti N, Marschall J, Drees M, et al. Strategies to prevent CLABSI in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. 2022;43(5):553–569. PMID 35437133.
- 11Lin MR, Chang PJ, Hsu PC, et al. Comparison of efficacy of 2% chlorhexidine gluconate-alcohol and 10% povidone-iodine-alcohol against catheter-related bloodstream infections and bacterial colonization at central venous catheter insertion sites. J Clin Med. 2022;11(8):2242. PMID 35456335.
- 12UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.