Central Venous Line
Removal.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
- Air embolism at IJ / SC is preventable with positioning + Valsalva + immediate occlusion.
- Negative intrathoracic pressure entrains air via the open venous tract — physiology is unforgiving.
- Femoral lacks air-embolism risk but carries retroperitoneal bleed risk, especially on anticoagulation.
- Anticoagulated patients double the femoral danger profile — pressure duration doubles per UCI protocol.
Mirski MA et al. Anesthesiology. 2007;106(1):164–77 · PMID 17197859
Site-specific risk.
Differentiate air-embolism risk at IJ / SC from retroperitoneal-bleed risk at femoral; explain the physiology of each.
Pre-removal eligibility.
Verify coagulation thresholds, anticoagulation hold, dwell days, and clinical-setting capacity before start.
Site-specific positioning.
Trendelenburg with head turned for IJ / SC; flat supine, hip neutral for femoral.
Valsalva-timed withdrawal.
Cue Valsalva (awake) or time to positive-pressure breath (ventilated) for IJ / SC; direct pressure for femoral.
Pressure duration.
5 min IJ / SC, 10 min femoral, doubled on therapeutic anticoagulation per UCI protocol.
Complication recognition.
Detect air embolism and retroperitoneal bleed; initiate Durant's maneuver, hold pressure, escalate cleanly.
- 01Line no longer indicated. No pressors, TPN, incompatible infusions, or dependence for poor peripheral access. Dwell days noted.
- 02Coag labs reviewed. PLT ≥ 50k IJ / SC · ≥ 100k femoral · INR ≤ 1.5. Anticoagulation held per protocol; last dose documented.
- 03Clinical setting confirmed. Monitored bed; bedrest capacity ≥ 2 h post-removal for femoral.
- 04Consent obtained. Plain-language: purpose, expected sensations (brief stinging), risks (bleeding, air embolism, fragmentation, site infection). Surrogate if patient lacks capacity.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, site, consent confirmed aloud. Team pause; re-verbalize before first incision into the dressing.
- Active bleeding from site without correctable cause
- Unable to obtain hemostasis with prolonged pressure
- Hemodynamic instability still requiring continued femoral access — preserve until alternative established
5–10 min hold for hemostasis · bedrest 1–2 h femoral · ambulate after IJ / SC · activity restrictions 24 h.
- Patient supine (flat) or 10–15° Trendelenburg
- Head turned away from insertion site
- Trendelenburg raises local CVP above atmospheric pressure
- Eliminates the atmosphere-to-vein pressure gradient
- Applies to IJ and SC sites only
- Confirm bed angle with visual or goniometer check — do not eyeball
Mirski MA et al. Anesthesiology. 2007;106(1):164–77 · PMID 17197859
Negative intrathoracic pressure on spontaneous inspiration creates an inward gradient at the open venous tract. Trendelenburg flips the gradient by raising CVP at the puncture site.
- Patient flat supine or minimally semi-supine
- Hip in neutral rotation — no external rotation
- Trendelenburg not indicated — no air-embolism risk at femoral site
- Patient remains supine ≥ 2 hours post-removal
- Ensure bedrest capacity before starting procedure
- Femoral site risk is hemorrhage, not air entrainment
Femoral vein sits below the right atrium · no atmosphere-to-vein gradient on inspiration · positioning is purely about access and post-removal bedrest.
dyspnea.
pain.
hypotension.
murmur.
- Full PPE: gown, mask, eye protection, sterile gloves
- CHG-alcohol skin prep around insertion site · allow appropriate dry time
- Remove existing dressing without traction on the catheter
- Cut anchoring suture wings with sterile scissors
- Avoid nicking catheter body during suture release — shearing risk
- Fenestrated sterile drape over prepared field
Pronovost P et al. N Engl J Med. 2006;355:2725–32 · PMID 17192537
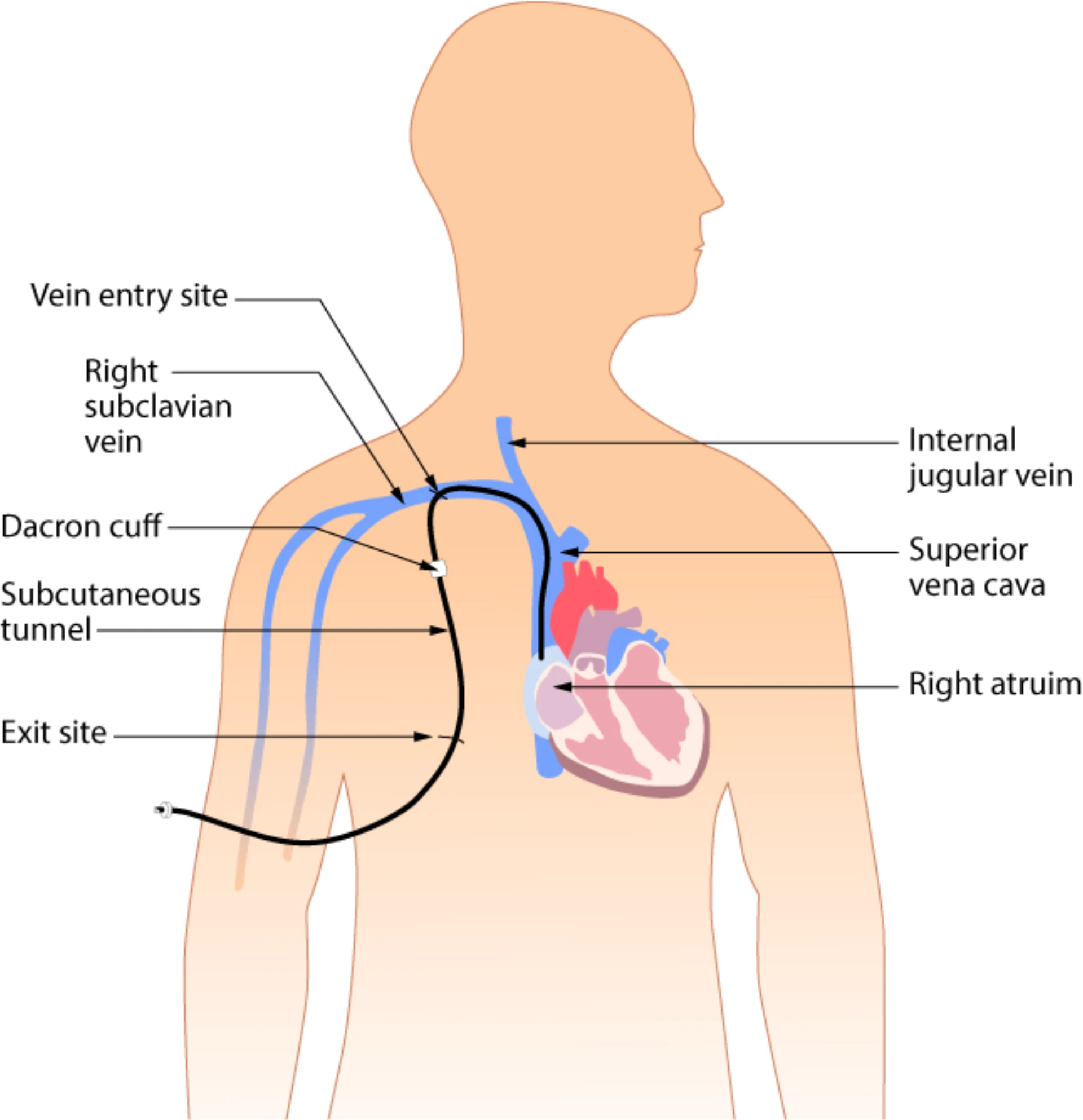
Wikimedia Commons · File: Tunneled venous access device.png · CC BY 4.0
Catheter exit-site and subcutaneous tunnel — anatomical orientation for suture release without traction.
Valsalva, slow steady withdrawal, immediate occlusion.
Cue Valsalva — bear down, exhale against a closed glottis. Increases intrathoracic pressure, raises CVP at the puncture site above atmospheric.
Time withdrawal to a delivered positive-pressure breath or end-inspiratory hold.
- Withdraw slowly and steadily during the Valsalva / positive-pressure phase
- Apply petrolatum-impregnated air-occlusive dressing the moment the catheter leaves the skin
- Do not pause mid-withdrawal — complete in one continuous motion
- No interval exposure of the venous tract to atmospheric pressure
Vesely TM. J Vasc Interv Radiol. 2001;12(11):1291–5 · PMID 11698628
Karlinskaya M et al. J Patient Saf. 2024;20(8):571–5 · PMID 39453709
- No Valsalva required at the femoral site
- Withdraw catheter slowly and steadily
- Apply two-finger direct manual pressure immediately on withdrawal
- Pressure proximal to skin puncture, over the femoral vein
- 10-minute minimum countdown begins at withdrawal
- Double to 20 min under therapeutic anticoagulation per UCI protocol
The 10-minute hold is a patient-safety element. If you must leave, hand off pressure with a clear timer to another qualified team member — do not shorten.
Tapered & intact — or escalate.
- Lay catheter flat on sterile drape
- Verify full catheter length intact
- Tapered distal morphology = intact
- Blunt · irregular · shortened = sheared → escalate
Send tip for culture only when CLABSI is clinically suspected — fever at removal, positive blood cultures, clinical deterioration. Routine tip culture is not recommended.
No bedside retrieval through the skin puncture.
Mermel LA et al. Clin Infect Dis. 2009;49(1):1–45 · PMID 19489710
Direct pressure over exit site.
5 min minimum, longer if oozing. Confirm hemostasis before dressing. SC harder to compress — watch for delayed hematoma.
Two-finger direct pressure.
10 min minimum proximal to skin puncture over the femoral vein. Continuous. No release at the 5-min mark.
Doubled — per UCI protocol.
20 min femoral, 10 min IJ / SC on therapeutic anticoagulation. Use a clock; document the duration.
- IJ / SC — petrolatum-impregnated gauze for tract sealing
- IJ / SC — sterile occlusive dressing over site for ≥ 24 h
- Femoral — sterile occlusive dressing + pressure-dressing reinforcement
- Transparent film allows site monitoring without removal
- Document dressing type and time applied
- Inspect site within 1 h for active bleeding
- Date, time, removal site (IJ / SC / femoral)
- Dwell days · anticoagulation status at removal
- Catheter length confirmed intact (or escalation noted)
- Positioning used · Valsalva performed (IJ / SC)
- Pressure duration (timed) · dressing type applied
- Complications · patient tolerance · post-removal vitals
- Post-removal orders: vitals q15 min × 1 h then q1 h × 4 h · 2 h supine bedrest femoral
Air embolism.
Sudden dyspnea, hypoxia, hypotension, mill-wheel precordial murmur. Left lateral decubitus + Trendelenburg (Durant's), 100% O2, rapid response call.
Retroperitoneal bleed.
Femoral site, often anticoagulated. Flank / back pain, hypotension, tachycardia, unexplained Hgb drop. Clean external dressing. Stat CBC + abdominopelvic CT, anticoagulation reversal, surgical / IR consult.
Catheter tip shear.
Blunt or shortened tip on inspection. Notify provider, stat CXR / abdominal film, IR consult for fragment retrieval. No bedside retrieval.
CRBSI on removal.
Send tip culture only if CLABSI clinically suspected (fever, positive blood cultures, clinical deterioration). Do not culture routinely — per CDC HICPAC 2011 and Mermel 2009 IDSA guidance.
Disclosure & family communication.
Timely, plain-language disclosure for any intra- or post-removal event. Document conversation, decisions, family present. Patient-safety officer per UCI policy.
Both scenarios.
Air-embolism arrest sequence and retroperitoneal-bleed escalation are drilled in the UCI Simulation Center per Stream-C gating.
Skipping Trendelenburg for IJ / SC.
Flat positioning eliminates the CVP-over-atmospheric gradient that prevents air entrainment. Always supine or 10–15° Trendelenburg, head turned, for IJ and SC.
Untimed pressure.
Eyeballed thirty seconds is not five minutes. Use a clock; document the duration. If you must leave, hand off pressure to a qualified team member with a timer.
Femoral removal · no AC hold plan.
No femoral removal on therapeutic anticoagulation without a doubled-pressure plan (20 min) plus post-procedure observation per UCI protocol.
Skipping tip inspection.
Always lay catheter on sterile drape and verify intactness. A sheared fragment missed at the bedside becomes a delayed Never Event when imaging finds it later.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of CVL Removal privilege | First 5 independent removals · ≥ 1 femoral (if privileged) · per-case review within 14 days · aggregate at 5 cases · close within 6 months |
| OPPE | Continuous baseline (TJC MS.08.01.03) | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication flag |
| Reinstatement | < 5 removals over 24 mo | Femoral: Stream C sim + 2 proctored femoral · IJ / SC: 1 proctored case per site · FPPE restarts |
| Ad-hoc FPPE | Sentinel event · peer concern · M&M | Any air embolism · RP bleed · retained fragment · 2 sheared tips in 90 d → focused review per §3 structure |
- Air-embolism occurrences · 0 per window
- Retroperitoneal-bleed occurrences (femoral) · 0 per window
- Retained catheter fragment · 0 (zero-tolerance)
- Site-appropriate positioning documented · 100%
- Site-appropriate pressure duration · 100% (tier-split)
- Valsalva / positive-pressure-breath documented IJ / SC · ≥ 95%
- Supine bedrest ≥ 2 h ordered for femoral · 100%
- Catheter tip inspection documented · 100%
- Tip culture stewardship · ≥ 95% with documented suspicion
- 01O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162–e193. PMID 21460264.
- 02Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the IDSA. Clin Infect Dis. 2009;49(1):1–45. PMID 19489710.
- 03Heckmann JG, Lang CJ, Kindler K, et al. Neurologic manifestations of cerebral air embolism as a complication of central venous catheterization. Crit Care Med. 2000;28(5):1621–5. PMID 10834723.
- 04Vesely TM. Air embolism during insertion of central venous catheters. J Vasc Interv Radiol. 2001;12(11):1291–5. PMID 11698628.
- 05Mirski MA, Lele AV, Fitzsimmons L, Toung TJK. Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007;106(1):164–77. PMID 17197859.
- 06Karlinskaya M, Scharf L, Sarid N. Knowledge and practices regarding prevention of central venous catheter removal-associated air embolism: a survey of nonintensive care unit medical and nursing staff. J Patient Saf. 2024;20(8):571–575. PMID 39453709.
- 07Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–32. PMID 17192537.
- 08Shah Z, Khan I, et al. Intraperitoneal hematoma after femoral catheterization: a case report and literature review. Cureus. 2022;14(5):e25140. PMID 35733506.
- 09Buetti N, Marschall J, Drees M, et al. Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. 2022;43(5):553–569. PMID 35437133.
- 10AHRQ. Making Healthcare Safer IV. AHRQ Publication. Rockville, MD; 2023.
- 11The Joint Commission. Universal Protocol UP.01.03.01 — pre-procedure verification, site marking, time-out. National Patient Safety Goals; 2024.
- 11aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 11bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 11cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 12The Joint Commission. IC.02.02.01 — infection prevention and control. Hospital Accreditation Standards; 2024.
- 13Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2024;47(1S):S1–S285.
- 14UCI APP Class 2 Training Plan Process. UCI Health Medical Staff Office. April 2026.
- 15DOP Revision Memo (NP/PA). UCI Department of Neurology. April 2026. §3, §5.