Lumbar Drain
Placement & Removal.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Lumbar_Drain_Learning_Objectives.docx
- Over-drainage subdural hematoma is the most dangerous complication — downward brain sag.
- Catheter-associated meningitis incidence rises sharply after 5 days of dwell time.
- Retained catheter fragments are 100% preventable with the never-withdraw-through-Tuohy rule.
- Post-dural puncture headache, nerve-root irritation, and CSF leak round out the morbidity profile.
Governale LS et al. Neurosurgery. 2008;63(4 Suppl 2):379–84
Anatomy & landmarks.
Conus medullaris terminates L1–L2; cauda equina within the lumbar cistern. Tuffier's line locates L3–L4 / L4–L5 — landmark accuracy ~70%.
Indications & thresholds.
SAH vasospasm, NPH workup, CSF leak, TAA/TAAA protection. Absolute contras: site infection, mass effect, uncorrected coagulopathy.
Tuohy insertion.
Bevel cephalad, midline, ~15° cephalad angle. Describe tactile feedback through skin → supraspinous → interspinous → ligamentum flavum → dura.
Catheter advancement.
5–7 cm into the subarachnoid space. Stop on lancinating radicular pain — withdraw to prior depth, never through the Tuohy.
Drainage system & tragus.
Level drip chamber to the external auditory meatus / tragus, zero the transducer, set ordered rate with hourly maximum.
Removal sequence.
4-h clamp trial · stable neuro exam · slow withdrawal · tip-completeness inspection · stop on resistance, consult neurosurgery.
- Aneurysmal SAH — vasospasm management / communicating hydrocephalus
- NPH diagnostic workup — high-volume drainage trial
- CSF-leak management — spontaneous intracranial hypotension; skull-base CSF rhinorrhea / otorrhea
- TAA / TAAA spinal-cord protection (perioperative)
- Idiopathic intracranial hypertension — salvage when refractory to medical therapy
Schievink WI. JAMA. 2006 · PMID 16705110 · Schlosser RJ, Bolger WE. Otolaryngol Clin North Am. 2006 · PMID 16757229
Leone N et al. J Vasc Surg. 2024 · PMID 38636609 · Zhou C et al. CNS Neurosci Ther. 2024 · PMID 39097911
- Absolute: localized infection at insertion site
- Absolute: mass effect / impending herniation / posterior-fossa lesion
- Absolute: uncorrected coagulopathy
- Platelets ≥ 100,000/µL elective · INR ≤ 1.4
- Intact skin at planned puncture site
- LP competency at UCI is a prerequisite — no LP, no lumbar drain
| Agent | Hold |
|---|---|
| Warfarin | Verify INR ≤ 1.4 before placement |
| LMWH prophylactic | ≥ 12 h since last dose |
| LMWH therapeutic | ≥ 24 h since last dose |
| DOAC | 48–72 h hold per renal function |
| Aspirin / NSAID | No mandated hold for monotherapy |
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
count + glucose.
pull or justify.
CSF pleocytosis.
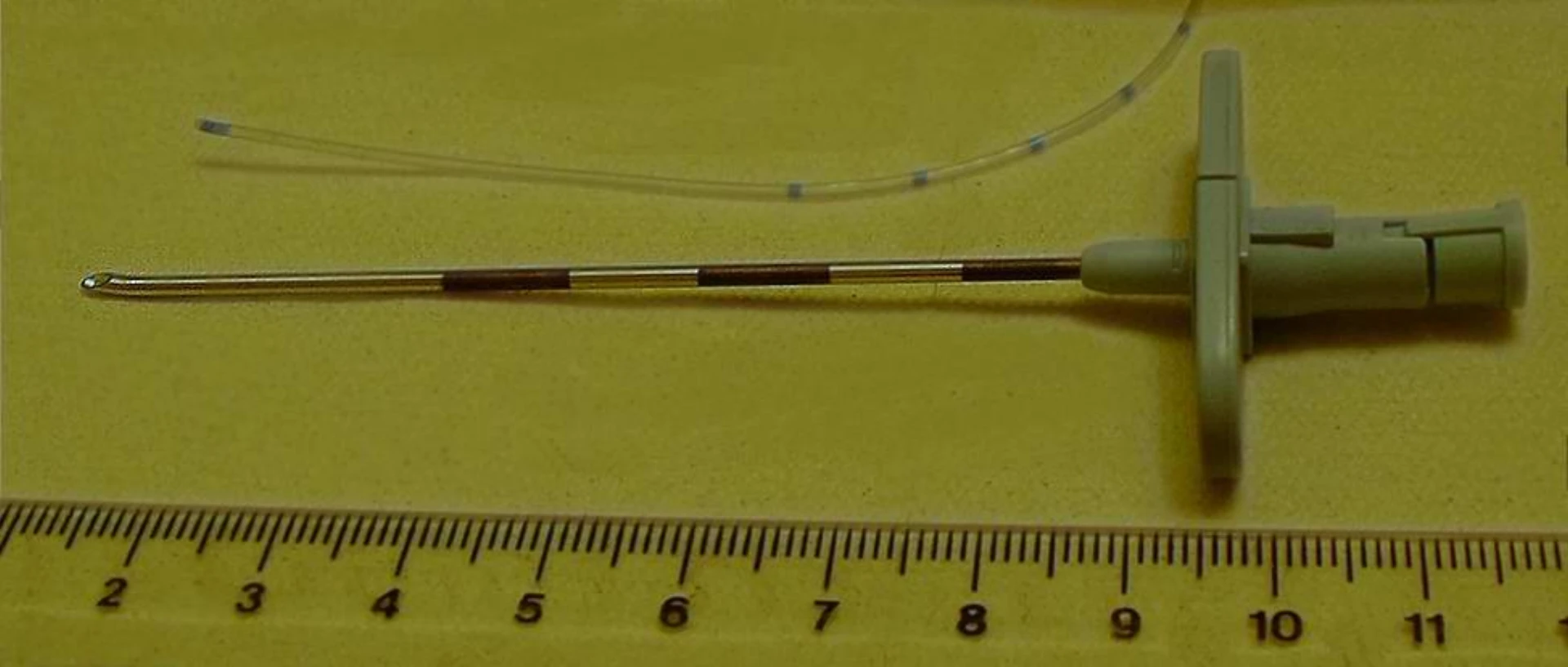
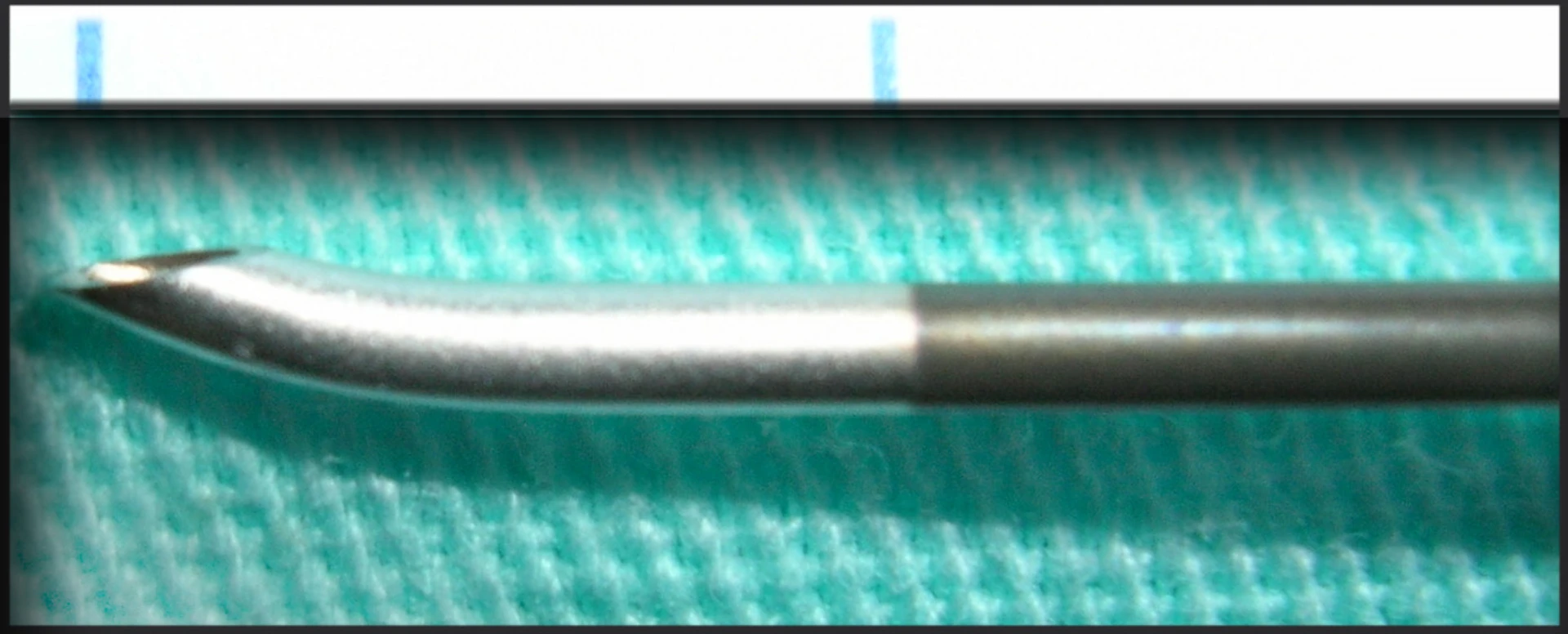
- Tuohy needle (curved-tip, cephalad bevel)
- Lumbar drainage catheter
- Luer connector + drip chamber + transducer
- Sterile preservative-free saline (priming)
- 1% lidocaine + 25g + 22g needles
- CHG-alcohol prep (or povidone-iodine alt.)
- Sterile gown, gloves, mask, eye protection
- Large fenestrated sterile drape
- Transparent occlusive dressing (Tegaderm)
- Suture (institutional protocol)
- Skin marker · ultrasound (if indicated)
- Specimen tubes for CSF
- Lateral decubitus — knees-to-chest, chin-tuck, spine maximally flexed
- Seated alternative — if lateral not tolerated; same flexion principle
- Tuffier's line — superior iliac crests → L3–L4 / L4–L5
- Landmark accuracy ~70% — Boon 2004
- Ultrasound when indicated: obesity · scoliosis · prior spine surgery · failed-LP history
- OPPE indicator: US use in indicated cases ≥ 95%

Position &
landmark.
- Lateral decubitus · knees-to-chest · chin-tuck · max flexion
- Tuffier's line — superior iliac crests
- Mark L3–L4 or L4–L5 interspace
- Ultrasound for obesity / scoliosis / prior surgery / failed-LP
Sterile field ·
anesthesia.
- Hand hygiene · gown · gloves · mask · eye protection
- CHG-alcohol prep · appropriate dry time · sterile drape
- 1% lidocaine — skin wheal then planned track
- Wait for onset before Tuohy advance
Tuohy ·
bevel cephalad.
- Midline approach · cephalad angle ~15°
- Tactile planes: skin → supraspinous → interspinous → lig. flavum → dura
- Dural "pop" — controlled, reliable in flexed lateral decubitus
- Bevel oriented cephalad for catheter direction
Confirm clear CSF
before you advance.
Withdraw the stylet at the hub. Clear CSF return at the hub is the gate. Document CSF appearance: clear, bloody, or xanthochromic.
Rotate bevel → advance 1–2 mm → withdraw slightly → redirect. Three-attempt ceiling at any one interspace, then move levels.
consult neurosurgery.
nerve-root injury and retained fragments.
Açıkbaş SC et al. Acta Neurochir. 2002;144:475–80
Catheter ·
5–7 cm.
- Advance 5–7 cm into subarachnoid space
- No excessive force at any plane
- Lancinating radicular pain → STOP, withdraw to prior depth
- NEVER withdraw catheter through Tuohy — shear risk.
Tuohy out ·
secure.
- Withdraw Tuohy over the catheter — never through
- Tunneled or sutured securement per institutional protocol
- Transparent occlusive dressing (Tegaderm)
- Document depth marker at skin
System ·
tragus level.
- Connect drainage system · prime with sterile saline
- Level drip chamber to external auditory meatus / tragus
- Zero the transducer · set ordered rate
- Hourly maximum — institutional cap 20 mL/h
- 01Clamp trial — 4 h. Clamp the drain · monitor for any neurological change · stable exam across the window is the gate.
- 02Sterile prep. CHG-alcohol prep at the site · sterile drape · gloves.
- 03Slow steady withdrawal. Do not yank · maintain axial alignment.
- 04Tip inspection. Inspect catheter tip for completeness — catch a retained fragment in the room, not on a CT three days later.
- 05Resistance → STOP. Do not pull harder. Consult neurosurgery · consider imaging before any further attempt.
- 06Occlusive dressing. Sterile occlusive dressing · monitor for CSF leak / PDPH.
- Strict supine bedrest · head of bed flat × 4 h
- Hourly neuro checks × 4 h, then per institutional protocol
- Hourly drain output charting · maximum drainage limit set
- No flushing · no manipulation by non-credentialed staff
- Notify MD for output change > 25%, new neuro change, or any CSF appearance change
- Daily CSF cell count + glucose if dwell > 72 h
- Day 5 — decision point: pull or justify in writing
Over-drainage SDH.
Downward brain sag → acute subdural hematoma. F-BEVAR SR/MA: CSFD-related mortality 1.4%, morbidity 25.6% (Leone 2024). Hard cap 20 mL/h.
Drain-associated meningitis.
Incidence rises sharply after 5 days. Pull drain · tip + CSF for culture + Gram stain · empiric vanc + cefepime (Tunkel 2017).
Post-dural puncture HA.
Pathogenesis = CSF hypotension. Supine rest, hydration, caffeine first-line. Epidural blood patch if refractory (Uppal 2024).
Radicular pain.
Lancinating leg pain on advance → STOP, withdraw to prior depth. Never through Tuohy — shear risk.
Retained fragment.
Withdraw catheter through Tuohy → bevel shears it. 100% preventable. IR retrieval ± surgical removal if it occurs (Açıkbaş 2002).
Spinal hematoma.
ASRA-5 holds prevent this. Warfarin INR ≤1.4, LMWH 12–24 h, DOAC 48–72 h (Kopp 2025).
Catheter migration.
Skin-marker depth change · plain film confirms position · do not flush a suspected occlusion (Açıkbaş 2002).
Dry tap.
3-attempt ceiling at one interspace. Rotate bevel · advance 1–2 mm · withdraw · redirect · move levels.
Withdrawing catheter through the Tuohy.
The bevel shears the catheter. You have a retained fragment in the patient. Withdraw the Tuohy over the catheter — never the reverse.
Drip chamber off the tragus.
Drip chamber not leveled to the external auditory meatus, or missing the hourly cap, drives over-drainage SDH. Re-zero on every reposition.
Pushing past a dry tap.
Three attempts is the ceiling at any one interspace. After that, move levels or escalate to neurosurgery — you do not keep stabbing.
Pulling on resistance during removal.
Resistance on withdrawal is a stop, not a tug. Forceful traction tears nerve roots and breaks catheters. Image · consult · do not improvise.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of LD privilege | First 5 independent cases · concurrent review within 14 d · aggregate at 5 cases · closed within 6 mo |
| OPPE | Continuous baseline · q6 mo | 10% sample (min 2, max 10) · 100% review on any complication · TJC MS.08.01.03 |
| Triggered FPPE | Severe complication · 2 failed placements / 90 d · RL Solutions event · M&M review | Scope per trigger · min 5 subsequent cases · §3 structure |
| Lapse / Reinstatement | < 3 cases over 24 mo | Simulation (Stream C) + 2 proctored cases · FPPE restarts on next 5 |
- Successful first-attempt placement ≥ 80%
- Ultrasound use in indicated cases ≥ 95%
- 100% review of any complication occurrence
- Documentation completeness 100% — time-out, consent, CSF, depth, orders
- Order-set adherence 100% — bedrest, neuro checks, hourly output, no-flush, notify
Declining output · new deficit.
Drain output drops from 10 mL/h to <2 mL/h over 3 h. Patient becomes lethargic with new right-sided weakness.
Best next step: Stop drainage · stat neuro exam · emergent non-contrast head CT. Not: flush, lower the chamber, or replace the drain.
Possible drain-associated meningitis.
Serosanguinous discharge, 2 cm halo erythema, fever 38.2 °C, slightly cloudy CSF from the drain.
Best next step: Remove the drain · catheter tip + CSF for culture & Gram stain · empiric vancomycin + cefepime pending results. Not: continue drainage on antibiotics.
Resistance during withdrawal.
Clamp trial × 4 h with stable exam. On withdrawal, sudden resistance at ~4 cm.
Best next step: STOP · do not pull harder · neurosurgery consult · consider imaging before further attempts. Not: firm steady traction, cut at skin, or saline lubrication.
- 01Açıkbaş SC, Akyuz M, Kazan S, Tuncer R. Complications of closed continuous lumbar drainage of cerebrospinal fluid. Acta Neurochir (Wien). 2002;144(5):475–480. PMID 12111503.
- 02Governale LS, Fein N, Logsdon J, Black PM. Techniques and complications of external lumbar drainage for normal pressure hydrocephalus. Neurosurgery. 2008;63(4 Suppl 2):379–384. PMID 18981847.
- 03Boon JM, Abrahams PH, Meiring JH, Welch T. Lumbar puncture: anatomical review of a clinical skill. Clin Anat. 2004;17(7):544–553.
- 04Wolf S, Mielke D, Barner C, et al. Effectiveness of Lumbar Cerebrospinal Fluid Drain Among Patients With Aneurysmal Subarachnoid Hemorrhage (EARLYDRAIN): A Randomized Clinical Trial. JAMA Neurol. 2023;80(8):833–842. PMID 37330974.
- 05Kopp SL, Vandermeulen E, McBane RD, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: ASRA Evidence-Based Guidelines (5th ed). Reg Anesth Pain Med. 2025. PMID 39880411.
- 06Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 IDSA Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin Infect Dis. 2017;64(6):e34–e65. PMID 28203777.
- 07Uppal V, Russell R, Sondekoppam RV, et al. Evidence-based clinical practice guidelines on postdural puncture headache: a consensus report from a multisociety international working group. Reg Anesth Pain Med. 2024;49(7):471–501. PMID 37582578.
- 08Leone N, Bath J, D'Oria M, et al. Systematic review and meta-analysis of cerebrospinal fluid drain-related mortality and morbidity after fenestrated-branched endovascular aortic repair. J Vasc Surg. 2024;80(2):586–594.e5. PMID 38636609.
- 09Lee Y, et al. Effectiveness of Cerebrospinal Fluid Lumbar Drainage Among Patients with Aneurysmal Subarachnoid Hemorrhage: An Updated Systematic Review and Meta-Analysis. World Neurosurg. 2024;183:246–253.e12. PMID 38246528.
- 10Lee Y, et al. The Benefits and Feasibility of External Lumbar Cerebrospinal Fluid Drainage for Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage: Meta-Analysis and Trial Sequential Analysis. World Neurosurg. 2022;167:e549–e560. PMID 35977676.
- 11Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006. PMID 16705110.
- 12Schlosser RJ, Bolger WE. Endoscopic management of cerebrospinal fluid rhinorrhea. Otolaryngol Clin North Am. 2006;39(3):523–538. PMID 16757229.
- 13Zhou C, et al. Progress and recognition of idiopathic intracranial hypertension: A narrative review. CNS Neurosci Ther. 2024;30(8):e14895. PMID 39097911.
- 14The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 14aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 14bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 14cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 14dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 14eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 14fThe Joint Commission. NPSG.03.05.01 EP 3 — perioperative management of patients on oral anticoagulants per approved protocols and evidence-based guidelines (bridging, hold timing, restart). Pairs with the ASRA-PM 5th-edition antithrombotic guideline cited above. National Patient Safety Goals (HAP); effective January 2025.
- 14gThe Joint Commission. NPSG.06.01.01 — clinical alarm safety; clinically appropriate settings, authority to change parameters, monitoring/response, and periodic accuracy checks for high-risk alarms. National Patient Safety Goals (HAP); effective January 2025.
- 15CDC. Guideline for hand hygiene in health-care settings. MMWR Recomm Rep. 2002;51(RR-16):1–45.
- 16Cook Medical. Tuohy epidural needle instructions for use. 2024 · Integra LifeSciences. Lumbar drainage system IFU. 2024.
- 17UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.