Arterial Line
Femoral.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/04_Arterial_Line_Femoral/
- Continuous invasive MAP is standard of care in aSAH with tight MAP targeting
- Tight SBP targets in hypertensive ICH require beat-to-beat pressure
- Post-arrest TTM with neuroprognostic MAP goals
- Status epilepticus requiring hemodynamic support during induction
- Failed radial access or radial perfusion inadequate in vasopressor-dependent shock
- Large caliber — reliable cannulation when peripheral pulses are weak
- Stability for transport in vasopressor-dependent shock
- Accessible during airway management without competition for upper-extremity real estate
- Complications are low frequency, high severity — retroperitoneal bleed, limb ischemia, pseudoaneurysm
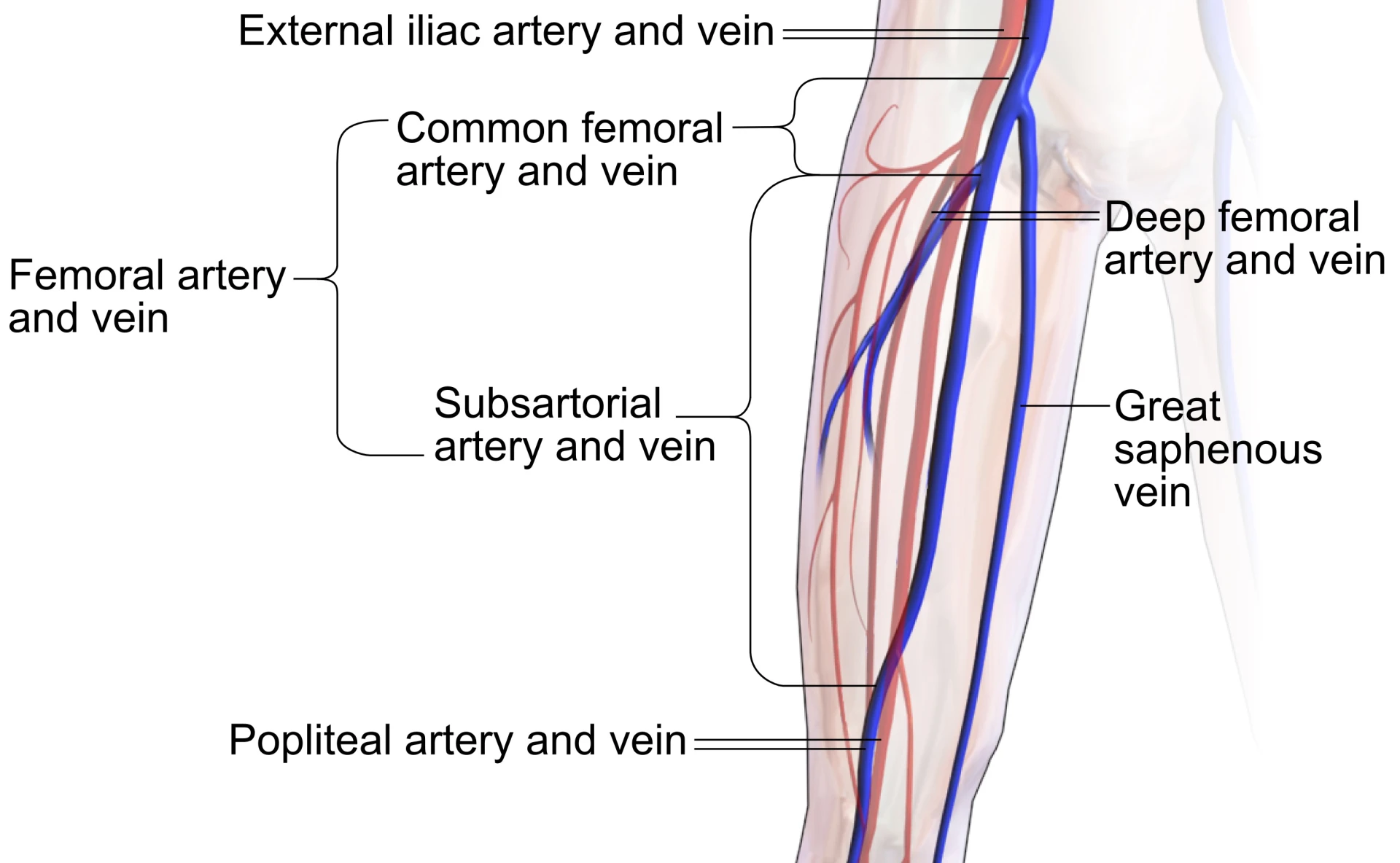
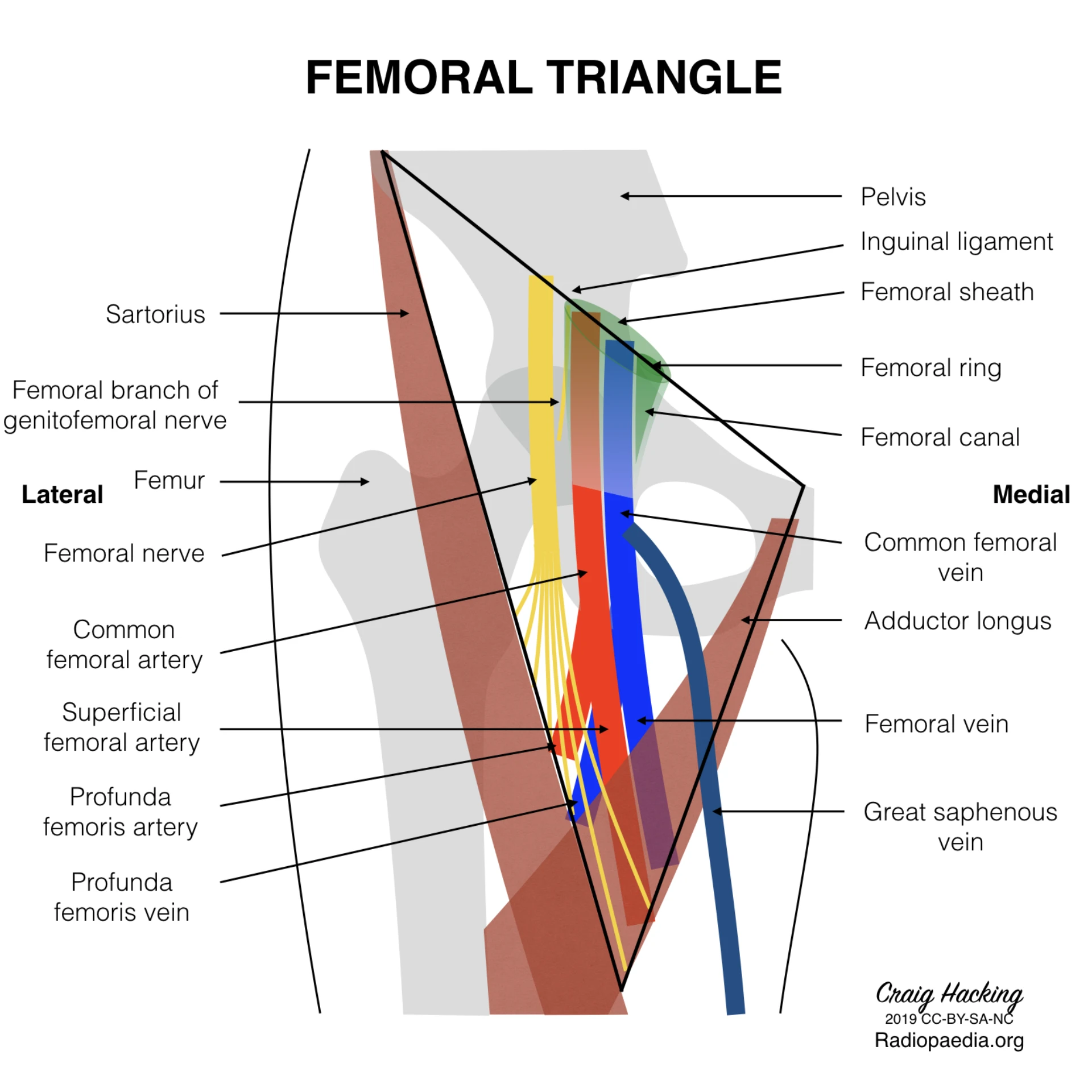
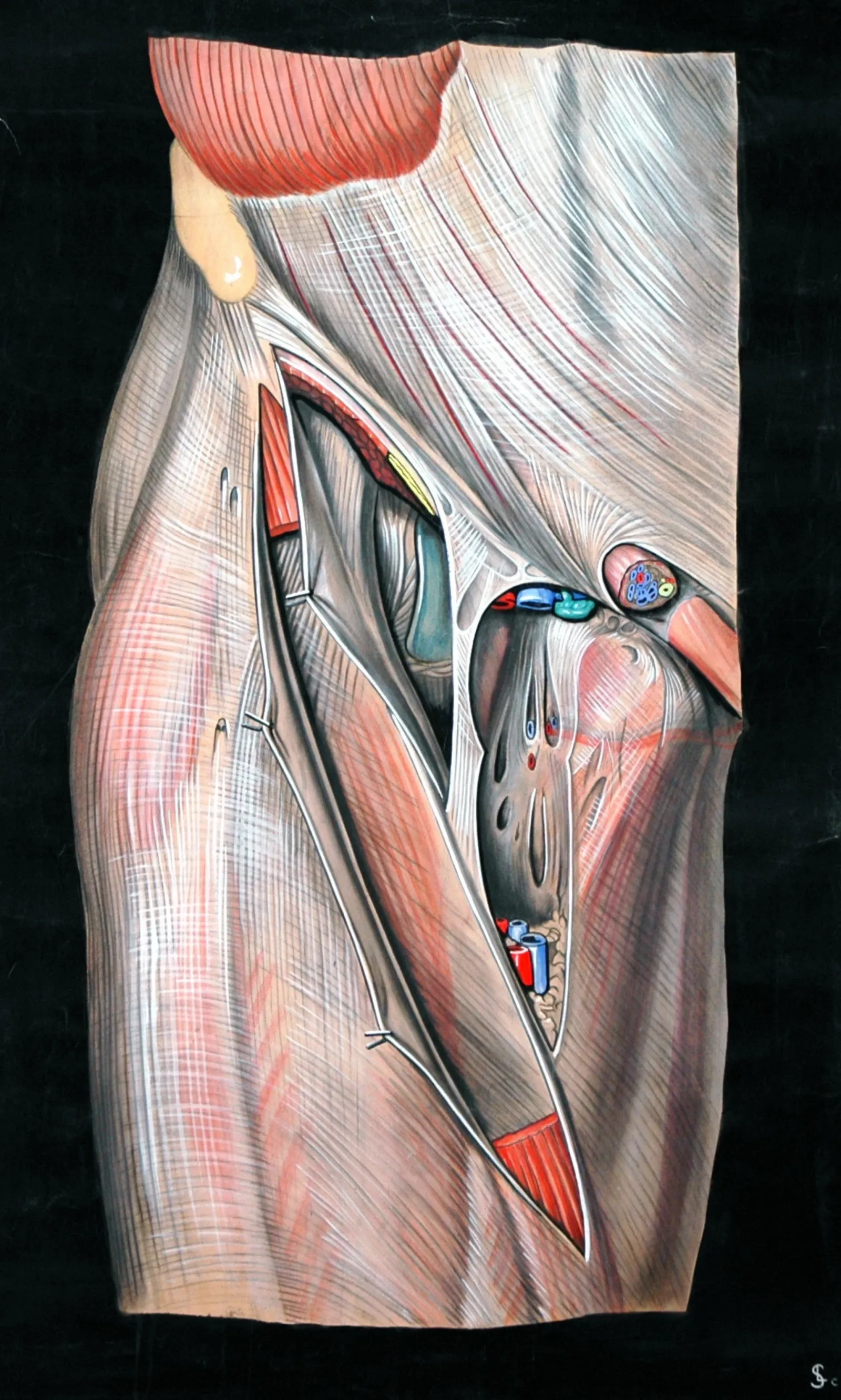
Femoral triangle anatomy.
Describe the NAVEL mnemonic lateral to medial — nerve, artery, vein, empty space, lymphatics — and recall why CFV sits medial to CFA at the inguinal ligament.
US discrimination.
Differentiate CFA from CFV on short-axis ultrasound: artery round, pulsatile, non-compressible; vein oval, compressible, thin-walled. Compressibility is the most reliable discriminator.
Seldinger cannulation.
Execute US-guided needle entry 1–2 cm caudal to inguinal ligament, pulsatile-return confirmation, wire-never-lost, catheter advancement, transducer setup.
Square-wave test.
Interpret the fast-flush test — optimal, over-damped, under-damped — and justify remediation for each state. Level transducer to phlebostatic axis.
Complication recognition.
Recognize retroperitoneal bleed, limb ischemia, pseudoaneurysm, AV fistula, CRBSI on clinical signs that mandate immediate escalation.
Appropriate escalation.
Escalate to neurointensivist, vascular surgery, or interventional radiology on defined clinical triggers — without attempting unilateral resolution.

- NFemoral nerve. Most lateral. Outside the femoral sheath — not our target, but anatomic landmark.
- ACommon femoral artery. Target vessel. Round, pulsatile, thick-walled, non-compressible.
- VCommon femoral vein. Medial to artery. Oval, compressible, thin-walled.
- EEmpty space (femoral canal). Loose connective tissue · lymph node of Cloquet.
- LLymphatics. Most medial. Empty into deep inguinal nodes.
| Finding | CFA | CFV |
|---|---|---|
| Shape | Round | Oval |
| Wall | Thick · hyperechoic | Thin |
| Pulsatility | Pulsatile | Non-pulsatile |
| Compressibility | Non-compressible | Collapses |
| Position | Lateral | Medial |
Scheer B et al. Crit Care. 2002;6(3):199–204 · PMID 12133178
- Severe hemodynamic instability requiring continuous MAP
- Tight BP targets — aSAH, hypertensive ICH, post-arrest TTM
- Frequent ABG sampling in respiratory failure
- Failed radial access or radial perfusion inadequate
- Vasopressor-dependent shock requiring transport stability
- Absolute: active infection at the femoral access site
- Absolute: ipsilateral vascular graft · recent ipsilateral vascular surgery
- Absolute: critical ipsilateral PAD · ipsilateral DVT
- Relative: severe coagulopathy not yet corrected · prior groin radiation · morbid obesity limiting US
- Non-emergent thresholds: plt ≥ 50,000/µL · INR ≤ 1.5
- Hold per ASRA-PM 5th ed (Kopp 2025) before non-emergent puncture
- 01Informed consent. Indication, risks (hematoma, retroperitoneal bleed, limb ischemia, infection, pseudoaneurysm, AV fistula), alternatives, right to refuse. Surrogate path when patient lacks capacity.
- 02Labs verified. Platelets ≥ 50,000/µL · INR ≤ 1.5 for non-emergent placement. Anticoagulant / antiplatelet status reviewed against ASRA-PM holds.
- 03US pre-scan completed. CFA position confirmed lateral to CFV. Patency verified. Depth from skin to anterior arterial wall noted.
- 04Laterality marked. R or L femoral marked on skin. Communicated to bedside RN and any assistant.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, side, equipment, consent confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
≥ 12/15
checklist
HIGH-risk gate
Independent ratings
- Integrated a-line kit (needle, J-wire, catheter)
- Pressurized saline flush transducer set
- High-frequency linear US transducer
- Sterile probe cover + sterile gel
- Chlorhexidine-alcohol skin antiseptic
- Full-barrier fenestrated sterile drape
- Cap, mask with face shield, sterile gown, gloves
- Suture or StatLock + transparent occlusive dressing
- Short-axis sweep of the femoral triangle
- Confirm CFA lateral to CFV (NAVEL orientation)
- Compressibility test — vein collapses, artery does not
- Assess for variant anatomy or high bifurcation
- Note depth from skin to anterior arterial wall
- Mark optimal entry point on skin
Prep ·
full barrier.
- Hand hygiene per WHO 5 Moments
- Cap, mask + face shield, sterile gown, gloves
- CHG-alcohol scrub, ≥30 s dry — do not blot, do not fan
- Full-body fenestrated sterile drape
- Sterile probe cover on linear US transducer
Local ·
1% lidocaine.
- 1% lidocaine without epinephrine
- Skin wheal at planned entry site
- Infiltrate along anticipated needle track
- Aspirate before each injection
- Allow 60–90 s for onset
Needle entry · below the inguinal ligament.
Confirm pulsatile arterial return
before you advance the wire.
Bright red, brisk, pulsatile flow in the needle hub. Dark non-pulsatile = venous: STOP, withdraw, hold pressure 5 min, re-scan CFA before reattempt.
Operator maintains physical grip on the wire at all times. Resistance on advance → stop, reconfirm position, redirect bevel. Never force.
Reposition needle, reconfirm pulsatile return, retry.
Scheer B et al. Crit Care. 2002;6(3):199–204 · PMID 12133178
Wire ·
J-tip first.
- J-tip first under operator control
- Smooth advance — never force
- Resistance → stop, reconfirm, redirect
- WIRE-NEVER-LOST
Catheter ·
over wire.
- Advance catheter into arterial lumen
- Retrieve wire intact
- Inspect for damage / deformation
- Confirm pulsatile return from catheter hub
Transducer ·
phlebostatic.
- Connect to primed pressure transducer
- Pressurized flush ~3 mL/hr
- Level to phlebostatic axis (4th ICS mid-axillary)
- Zero to atmosphere · luer-lock all
Square-wave ·
read the damping.
- Optimal: 1–2 brisk undershoot oscillations
- Over-damped: slurred, blunted — air, kink, clot, loose
- Under-damped: exaggerated, spuriously tall peaks
- Diagnose damping before treating the number
- Suture or manufacturer securement device (StatLock) at hub
- Transparent occlusive dressing per Buetti 2022 SHEA update — site visible
- Label dressing — date, time, initials
- Confirm waveform stable on monitor before leaving bedside
- Indication · consent · time-out · side
- US use · # punctures · entry below inguinal ligament
- Pulsatile confirmation · wire-advance under control
- Catheter gauge / length · waveform status · square-wave
- Complications · post-procedure orders
- Pressurized flush at ~3 mL/hr continuous
- Limb checks q1h × 4h then per unit protocol — distal pulses, color, cap refill, sensation
- Dressing check q shift — intact, dry, no bleeding
- Waveform quality reassessed each shift
- Removal criteria + hold parameters documented
- Damping change · weak distal pulse
- Expanding groin mass · flank or back pain
- Hemodynamic instability · hemoglobin drop
Retroperitoneal hemorrhage.
Flank/back pain, hypotension, Hgb drop, clean groin exam. CT angio · vascular surgery · hold anticoagulants · MTP if unstable.
Pseudoaneurysm.
Palpable thrill, expanding pulsatile mass. Confirm with US Doppler · vascular consult.
AV fistula.
New bruit at groin, machinery murmur. Confirm with US Doppler · vascular consult.
Distal limb ischemia.
Cold, mottled limb · weak DP/PT · cap refill >3 s. Remove line · vascular surgery emergent.
Catheter-related BSI.
CHG-alcohol prep, sterile barrier, daily necessity review. Same antiseptic discipline as CVL.
Local hematoma.
Expanding groin mass post-removal. Manual pressure ≥10 min · longer if anticoagulated.
Femoral thrombosis.
Higher with prolonged dwell. Daily review for necessity. Remove when no longer needed.
Wrong-vessel cannulation.
Dark, non-pulsatile return. STOP, withdraw, hold pressure 5 min, re-scan CFA before reattempt.
Kopp SL, Vandermeulen E, McBane RD, et al. Reg Anesth Pain Med. 2025 · PMID 39880411
Wrong vessel — venous puncture.
Dark, non-pulsatile return. STOP. Withdraw and hold pressure 5 min. Re-scan to confirm CFA before reattempt.
High puncture above the ligament.
Risks retroperitoneal hemorrhage. Stay 1–2 cm caudal to the inguinal ligament; midpoint ASIS–pubic tubercle on US.
Wire won't advance — force applied.
Force = wrong space or against vessel wall. Reposition needle, confirm pulsatile return, never push the wire.
Damped trace not investigated.
Square-wave test missed. Air, kink, clot, loose connection, low bag pressure, level off. Diagnose damping before treating the number.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of A-line Femoral privilege | First 5 independent cases · concurrent review within 14 d · aggregate at 5 cases · close within 6 mo |
| OPPE | Continuous baseline · TJC MS.08.01.03 | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication flag |
| Triggered | Severe event · ≥2 failures in 90 d · safety report · M&M | Ad-hoc focused review per §3 structure · minimum 5 subsequent cases |
| Lapse | < 3 lines over 24 mo rolling | Sim Stream C + 2 proctored live cases rated Independent |
- First-attempt success ≥ 80%
- US-guided placement ≥ 95% overall · 100% in obesity / hypotension / weak pulse / failed radial
- Limb complication rate target < 2%
- Square-wave optimal at 24 h ≥ 90%
- CRBSI rate target < 1 per 1,000 catheter-days
- Documentation completeness 100%
- 01Scheer B, Perel A, Pfeiffer UJ. Clinical review: complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care. 2002;6(3):199–204. PMID 12133178.
- 02Brzezinski M, Luisetti T, London MJ. Radial artery cannulation: a comprehensive review of recent anatomic and physiologic investigations. Anesth Analg. 2009;109(6):1763–81. PMID 19923502.
- 03Kopp SL, Vandermeulen E, McBane RD, Perlas A, Leffert L, Horlocker T. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: ASRA-PM Evidence-Based Guidelines (5th ed). Reg Anesth Pain Med. 2025. PMID 39880411.
- 04Buetti N, Marschall J, Drees M, et al. Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. 2022;43(5):553–569. SHEA/IDSA. PMID 35437133.
- 05Standring S, Tubbs SR (eds). Gray's Anatomy: The Anatomical Basis of Clinical Practice. 43rd ed. Elsevier; 2025.
- 06The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 06aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 06bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 06cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 06dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 06eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 06fThe Joint Commission. NPSG.06.01.01 — clinical alarm safety; clinically appropriate settings, authority to change parameters, monitoring/response, and periodic accuracy checks for high-risk alarms. National Patient Safety Goals (HAP); effective January 2025.
- 06gThe Joint Commission. NPSG.02.03.01 EP 1 — report critical results of tests and diagnostic procedures within an established time frame; written procedures define which results are critical and to/from whom they are reported. National Patient Safety Goals (HAP); effective January 2025.
- 07The Joint Commission. Infection Prevention and Control. Standard IC.02.02.01; 2024.
- 08The Joint Commission. Human Resources. Standards HR.01.06.01 (initial competence) and HR.01.07.01 (ongoing competence, ≥3-yr cycle). 2024. (Per CITATION_AUDIT 2026-04-28, HR.01.06.03 was removed; its substance is split between HR.01.06.01 and HR.01.07.01.)
- 09The Joint Commission. Medical Staff. Standards MS.06.01.05 (objective evidence-based privilege evaluation), MS.08.01.01 (FPPE — required for all new privileges), and MS.08.01.03 (OPPE — codified ≤ 12-mo cycle). 2024. (Per CITATION_AUDIT 2026-04-28, the FPPE substance lives at MS.08.01.01, not MS.07.01.01.)
- 10California Code of Regulations. Title 16, §1474 (BRN standardized procedures); §1399.541 (PA performable medical services).
- 11CMS Conditions of Participation. 42 CFR §482.12(a)(6) (privileges based on individual competence) and §482.22(c)(6) (bylaws include privilege criteria).
- 12UCI APP Class 2 Training Plan Process. University of California, Irvine Health. April 2026.
- 13UCI FPPE Master Plan §5. University of California, Irvine Health. April 2026.
- 14Strauss SA, Ma GW, Seo C, et al. Ultrasound-guided versus anatomic landmark-guided percutaneous femoral artery access. Cochrane Database Syst Rev. 2025;3:CD014594. PMID 40152297.