Arterial Line
Radial.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/05_Arterial_Line_Radial/
- Default arterial site — continuous MAP in aSAH, ICH, TTM, status epilepticus.
- Lower complication profile than femoral in most patients.
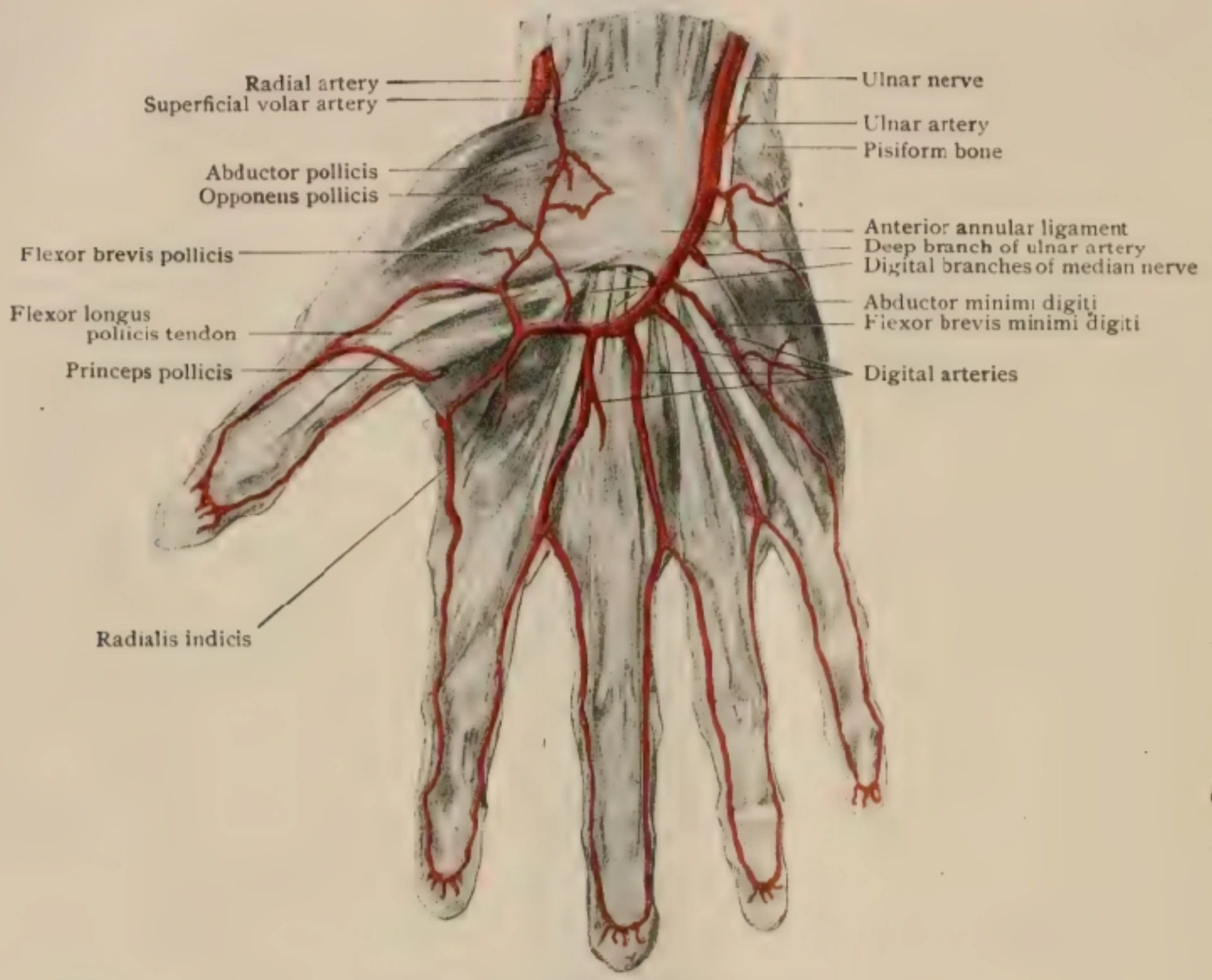
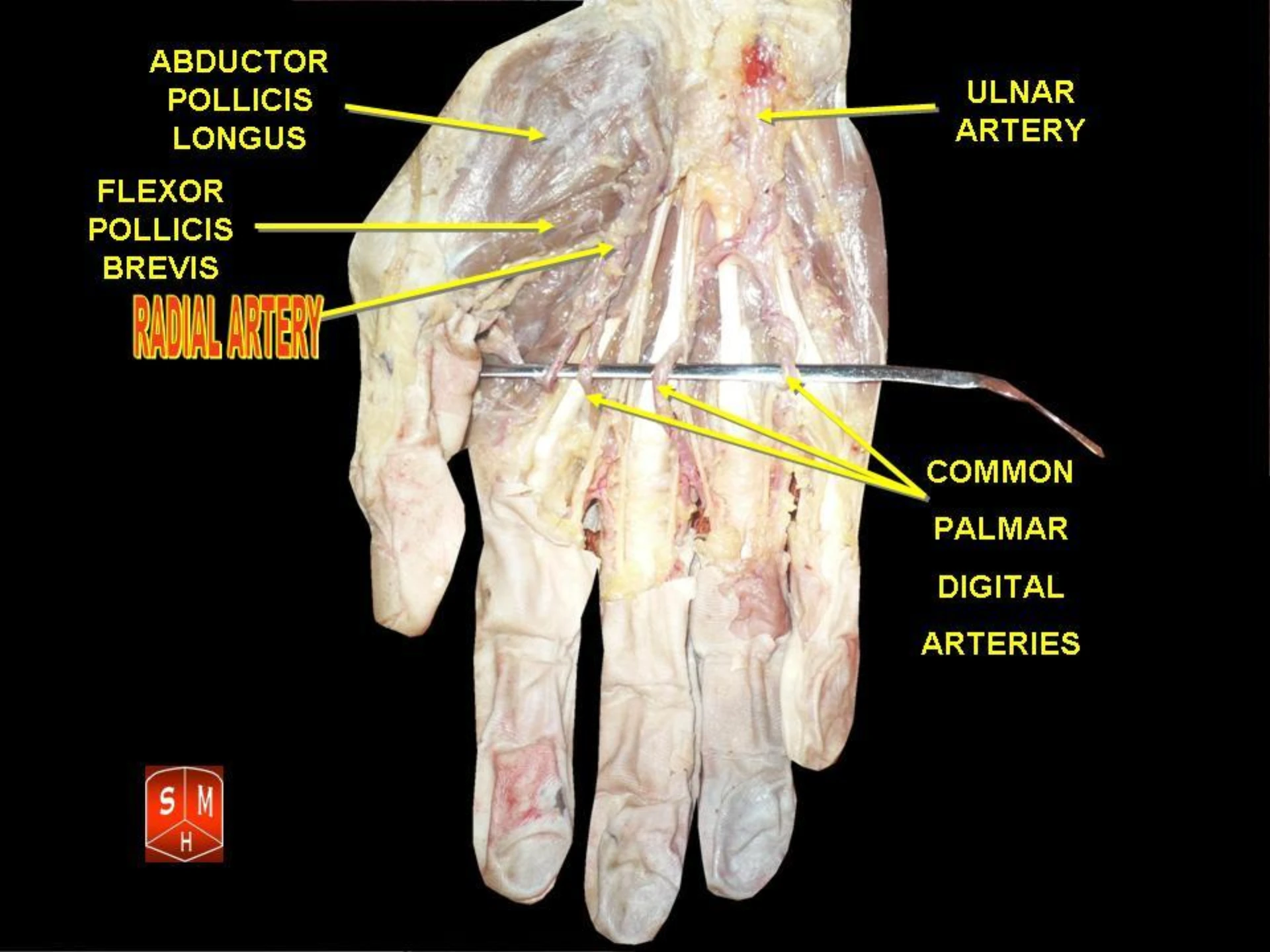
- Reliable ulnar collateral via the deep + superficial palmar arches.
- Frequent ABG sampling without repeated arterial puncture.
- Femoral fallback when shock, weak pulse, or failed radial attempts dictate.
Brzezinski M, Luisetti T, London MJ. Anesth Analg. 2009;109(6):1763–81 · PMID 19923502
Indications & contraindications.
Pressor titration, hypertensive emergency, frequent ABGs, beat-to-beat MAP monitoring; absolute and relative contraindications.
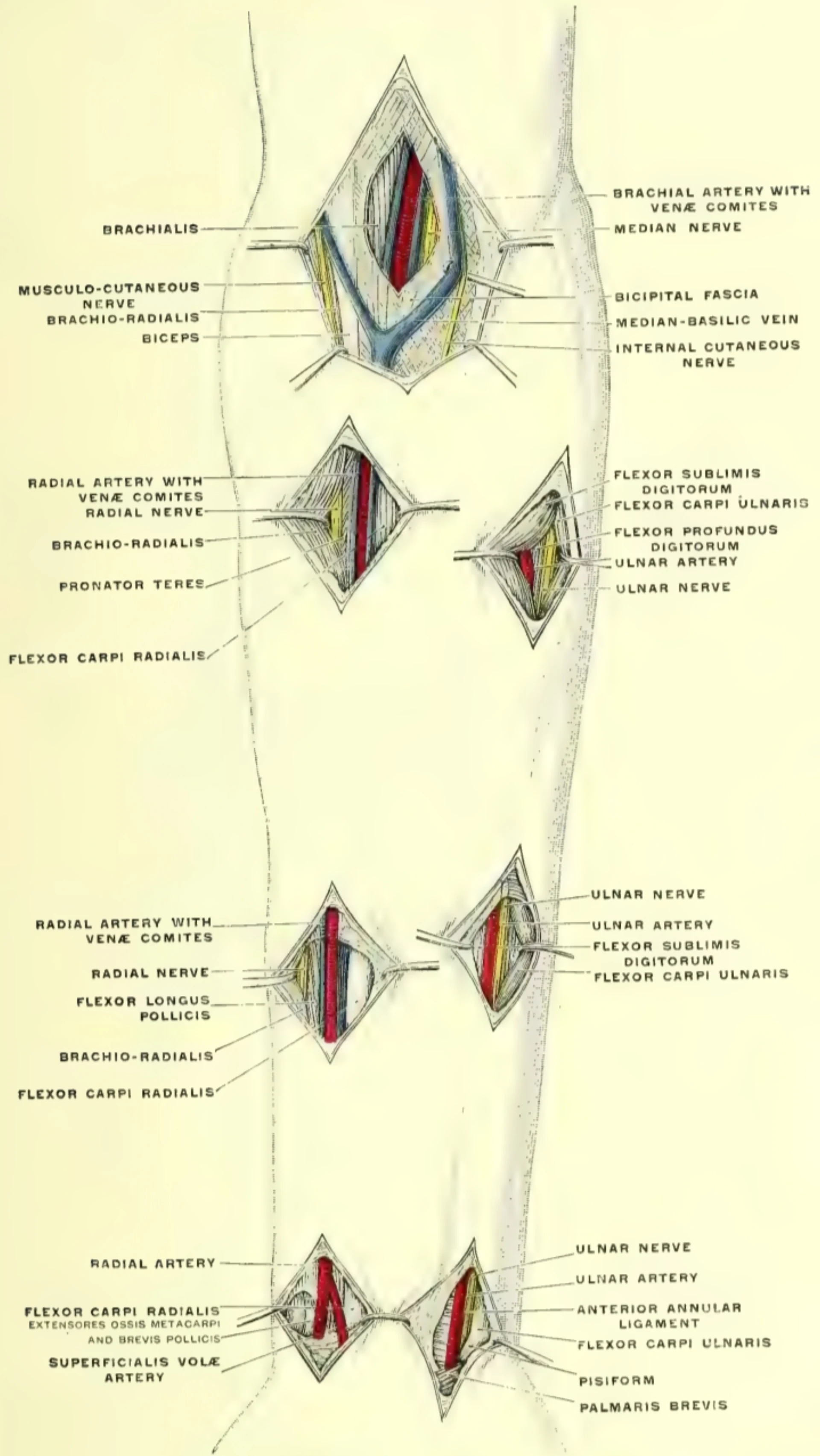
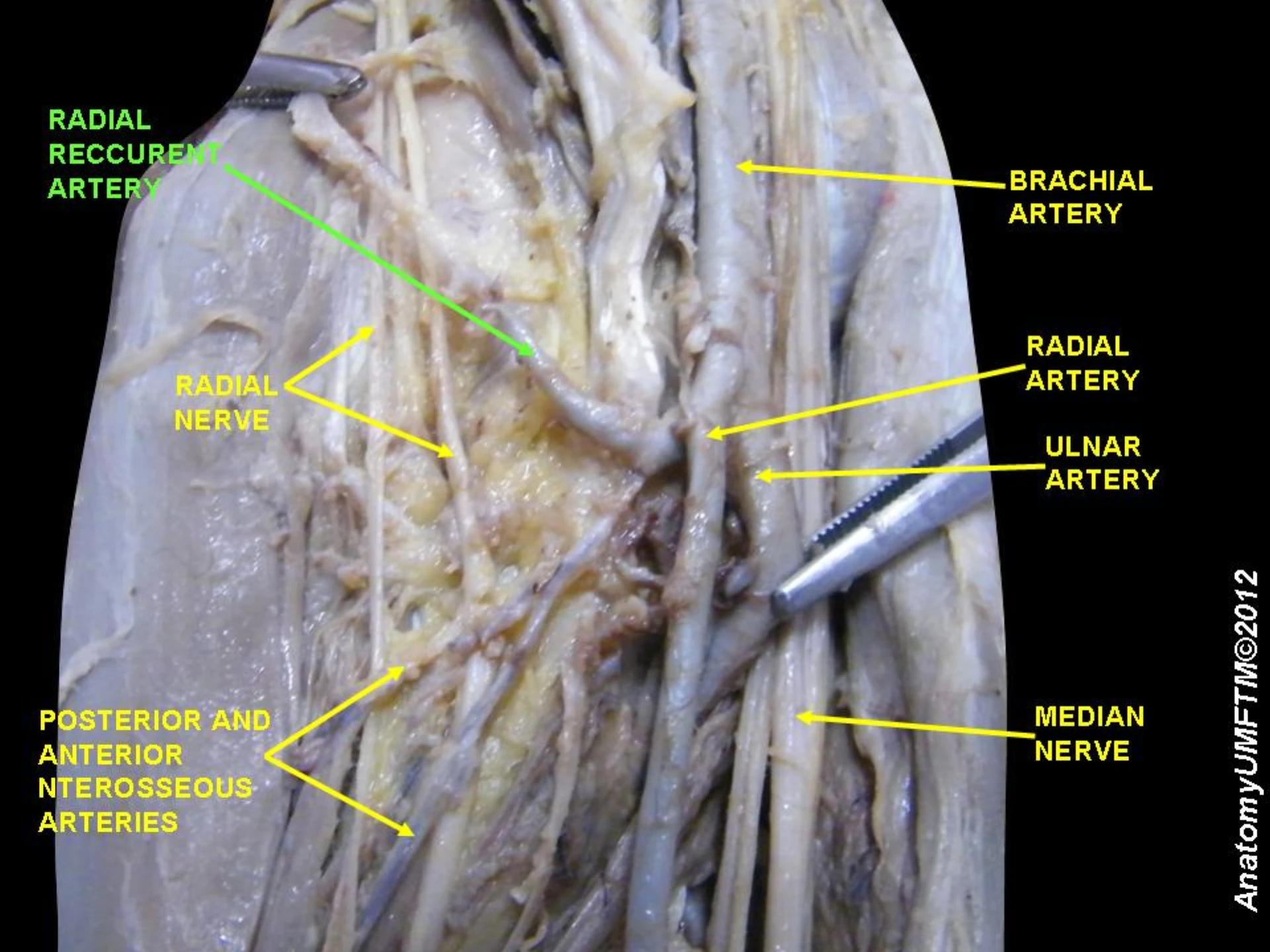
Anatomy & collateral flow.
Radial artery course at the wrist; ulnar collateral via the deep + superficial palmar arch; documentation as the standard.
US-first technique.
Short-axis at the wrist; long-axis in-plane for real-time needle-tip tracking; preferred over modified Allen alone.
Transducer setup.
Level to the phlebostatic axis · zero to atmosphere · square-wave damping check before any titration.
Waveform interpretation.
Recognize over- and under-damped tracings; correlate with cuff pressure on discordance; do not treat artifact.
Complication recognition.
Occlusion, distal ischemia, hematoma, nerve injury — hourly perfusion check, remove early, escalate cleanly.
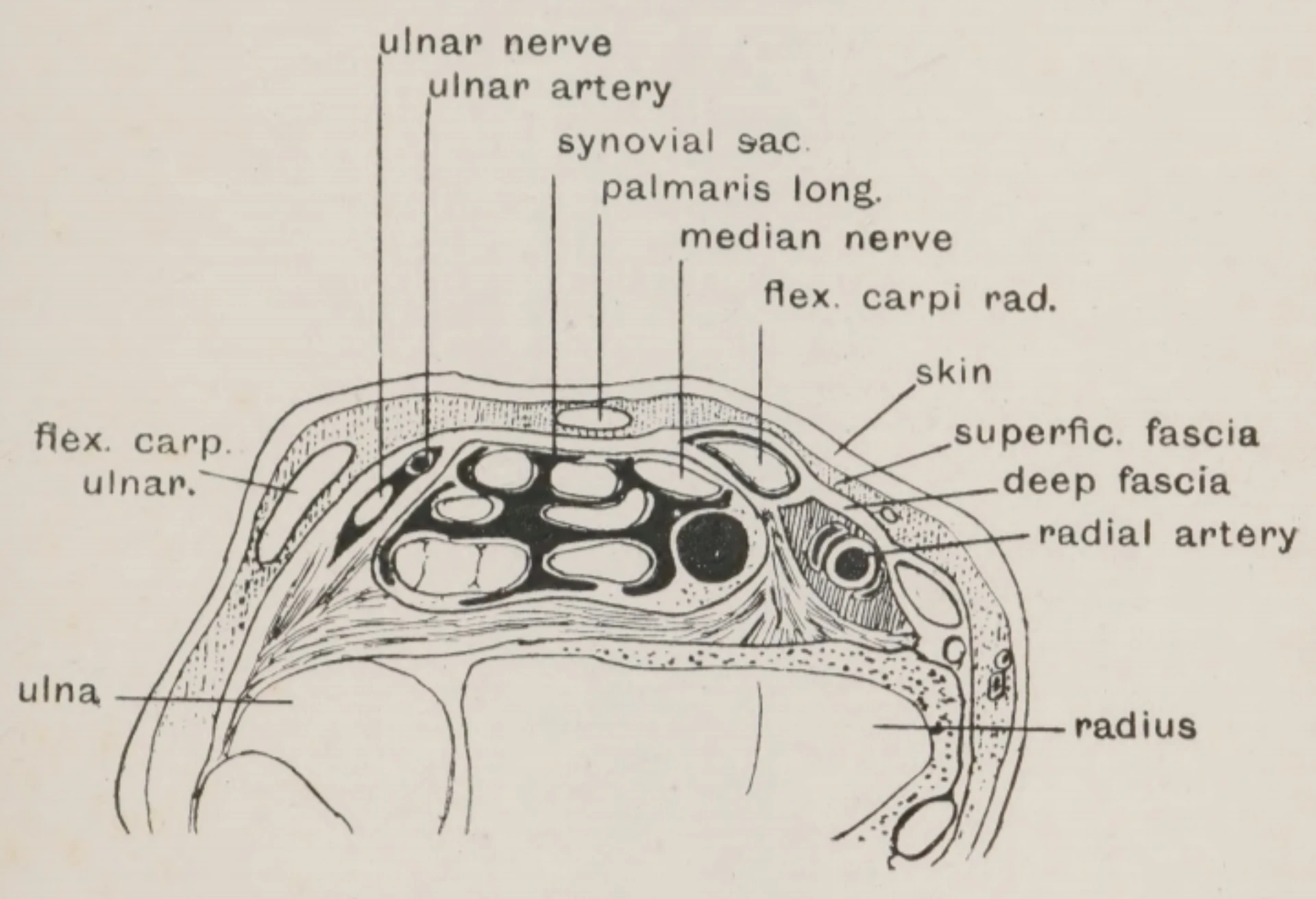
- Artery courses between FCR tendon (medial) and the distal radius (lateral)
- Palmar to the radial styloid process
- Paired venae comitantes flank the artery
- Superficial branch of the radial nerve runs deep and lateral
- Deep palmar arch supplies ulnar collateral to the hand
- Most superficial and accessible at the distal ventral wrist
- Radial artery — pulsatile, round, thick-walled, non-compressible
- Venae comitantes — paired, thin-walled, compressible under probe pressure
- FCR tendon — echogenic fibrillar structure medial to the artery
- Distal radius — posterior acoustic shadow as deep landmark
- Color Doppler confirms arterial pulsatility in weak-pulse or hypotensive patients
Weak or impalpable pulse · obesity · vasopressor-dependent shock · edema · prior failed landmark attempts. Long-axis in-plane once short-axis localization is established — real-time needle-tip tracking reduces posterior-wall transfixion.
- 01Modified Allen test. Compress radial + ulnar · clench & blanch palm · release ulnar · flush in < 6 s = adequate collateral. Sensitivity is poor — used alone it does not exclude ischemia risk.
- 02POCUS ulnar Doppler. Color Doppler over the deep palmar arch with radial compression confirms ulnar inflow. Modern standard for collateral assessment per Shiloh 2011.
- 03Clinical-judgment note. When neither is feasible, an explicit clinical judgment note in the pre-procedure record satisfies the documentation requirement.
Documentation of a collateral flow assessment — by Allen, POCUS, or clinical-judgment note — is the standard. Pass/fail of the Allen test alone is not.
- Tight MAP control — aSAH, ICH, hypertensive emergency
- TTM and post-arrest neuroprognostication
- Status epilepticus on continuous infusions / pressors
- Frequent ABG sampling — pressor or vent titration
- Default first site when collateral is intact and wrist accessible
Brzezinski M et al. Anesth Analg. 2009;109(6):1763–81 · PMID 19923502
- Absolute: inadequate ulnar collateral · active infection at site
- Absolute: Raynaud · Buerger · vasculitis
- Absolute: ipsilateral AV fistula or planned dialysis access
- Absolute: prior ipsilateral radial harvest (CABG)
- Relative: severe vasoconstriction on high-dose pressors · severe coagulopathy
- ASRA holds: ASA continue · clopidogrel 7d · UFH 4–6h · LMWH prophy 12h / Tx 24h · DOACs 48–72h · INR ≤ 1.4 elective
- 01Informed consent. Indication · femoral-fallback alternative · material risks (thrombosis, hematoma, ischemia, nerve injury) · refusal pathway acknowledged. Surrogate when patient lacks capacity.
- 02Labs reviewed. Platelets · INR · PTT. Apply ASRA holds for antithrombotics.
- 03Collateral flow documented. Allen, POCUS, or clinical-judgment note — recorded in pre-procedure note.
- 04Laterality confirmed. Left wrist vs right wrist — stated aloud. This is the named safety focus for the lateralized procedure.
- 05Team time-out. Per TJC UP.01.03.01 — correct patient, procedure, side, equipment, consent. Transducer primed · flush bag pressurized to 300 mmHg.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
If a complication occurs — bedside disclosure to patient + family within 24 h per UCI policy.
- Integrated radial a-line kit (Seldinger)
- Or over-the-needle cannula (transfixion)
- Chlorhexidine-alcohol prep stick
- Sterile fenestrated drape
- 1% lidocaine · 25g needle · 3 mL syringe
- Pressurized flush transducer set (primed)
- Pressure bag at 300 mmHg · ~3 mL/hr
- Suture or StatLock securement
- Transparent occlusive dressing (CHG-impregnated)
- Linear high-frequency US probe · sterile sleeve · gel
- Linear high-frequency probe (vascular preset)
- Short-axis confirms pulsatility + non-compressibility (artery) vs paired compressible veins
- Identify FCR tendon medial · distal radius shadow deep
- Map artery depth, diameter, anatomic variants
- Color Doppler for weak-pulse / hypotensive cases
- Mark skin entry under probe footprint
Position ·
wrist on a roll.
- Arm supinated on flat surface
- Wrist extended 30–45° over a folded towel roll
- Forearm secured to armboard / bed
- Fingers exposed for distal perfusion checks
- Identify radial pulse at maximum impulse
Prep & drape ·
sterile field.
- Hand hygiene · sterile gloves · mask · eye protection
- CHG-alcohol prep — scrub 30 s · dry 2 min
- Sterile fenestrated drape over wrist
- Sterile probe cover when US is used
- Maintain sterile field throughout
Local anesthesia ·
shallow wheal.
- 1–2 mL of 1% lidocaine in a 3 mL syringe
- 25g needle for the skin wheal
- Infiltrate over the palpated pulse
- Small subcutaneous only — avoid deep injection
- Wait 60 s for anesthetic onset
Pulse · US
localization.
- Palpate point of maximum impulse
- Pre-scan short-axis to confirm artery
- Doppler for weak-pulse / shock
- Mark position + depth
- Long-axis in-plane for needle-tip tracking
Needle entry ·
30–45°.
- 30–45° angle to skin
- Steeper under US short-axis
- Shallower for landmark / palpation
- Advance slowly
- Two approaches: Seldinger vs transfixion
Pulsatile
return.
- Bright-red, pulsatile flash at hub
- Stabilize the needle — do not advance
- Confirm: pulsatile + bright red
- Differentiate from venous (dark, non-pulsatile)
- WIRE-NEVER-LOST if Seldinger.
Prove the waveform is real
before you titrate.
Sharp systolic upstroke · dicrotic notch visible · 1–2 brisk undershoots after the square-wave release. Proceed.
Blunted upstroke · absent dicrotic notch · no oscillations. Underestimates systolic, overestimates diastolic. Check air in tubing, kinks, clots, loose connections, catheter against vessel wall.
Exaggerated upstroke with ringing · > 2 oscillations. Overestimates systolic. Shorten or stiffen tubing · remove stopcocks · re-prime. Do not treat the spuriously high systolic.
Zero to atmosphere. Re-level on position change.
Scheer B et al. Crit Care. 2002;6(3):199–204 · PMID 12133178
- Seldinger: advance J-tip wire smoothly · no force on resistance · wire-never-lost
- Thread catheter over wire into the artery · withdraw wire in one motion
- Transfixion: deliberately through both walls · remove stylet · slowly withdraw catheter until pulsatile flashback returns
- Advance catheter into the lumen · confirm pulsatile blood return
- Suture or StatLock securement at the hub
- Transparent occlusive dressing over insertion site
- Fingers exposed · wrist immobilizer optional for restless patients
- Immediate distal perfusion check — pulse · color · temperature · capillary refill at thumb and index
- Order set: continuous pressurized flush · q1h perfusion checks × 4h · escalation parameters
| Complication | Incidence | Recognition | Action / escalation |
|---|---|---|---|
| Thrombosis · occlusion | ~20% asymptomatic, transient | Loss of waveform · loss of pulse on removal | Smaller catheter + shorter dwell lower risk · usually silent + self-resolves. |
| Hand · digit ischemia | < 1% symptomatic | Pallor · pain · paresthesia · loss of pulse · delayed capillary refill at thumb / index | Immediate removal · direct pressure · attending + vascular surgery consult if not resolving. |
| Hematoma | Common · usually minor | Swelling · bruising at site | Direct pressure ≥ 5 min post-removal · longer if anticoagulated · mark and re-check. |
| Infection · CRBSI | Rare · < 1 / 1,000 catheter-days target | Site erythema · purulence · positive cultures | Sterile technique + CHG-alcohol prep + daily review per CDC 2011. |
| Radial nerve injury | Zero tolerance | New radial-distribution sensory or motor deficit | Remove line · document · neurology consult · triggers focused review. |
| Pseudoaneurysm · AV fistula | Late vascular | Pulsatile mass · bruit post-removal | Vascular ultrasound · surgery consult. |
Under-damped waveform missed.
A spuriously elevated systolic gets treated. Square-wave test on every connection and every shift. If the invasive reading disagrees with the cuff by > 20 mmHg, trust neither until you re-prove the system.
Failure to re-level the transducer.
Patient repositioned, bed lowered, transducer never moved — your MAP is wrong. Re-level to the phlebostatic axis after any position change.
Allen test alone for collateral.
The modified Allen test has poor sensitivity. Where POCUS is feasible, POCUS Doppler of the deep palmar arch is the modern standard. Documentation is the requirement — not a pass / fail score.
Late removal on distal ischemia.
Pallor, pain, paresthesia, loss of pulse — remove first, escalate second. The catheter is replaceable. The hand is not.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of radial A-line privilege | First 3 independent cases · concurrent review within 14 d · aggregate at 3-case completion · close within 6 mo |
| OPPE | Continuous baseline · q6 mo (TJC MS.08.01.03) | 10% sample (min 2 · max 10) · 100% review on any complication flag |
| Triggered FPPE | Hand ischemia · nerve injury · CRBSI · ≥ 2 failed in 90 d | Ad-hoc focused review · 3 subsequent cases · a/b/c outcome |
| Reinstatement | < 3 cases / rolling 24 mo | Stream B + 1 proctored case rated Independent |
- First-attempt success ≥ 70% (radial baseline)
- US used ≥ 80% overall · 100% in shock / weak-pulse / obesity / 2 failed landmark
- Symptomatic thrombosis < 2% · hand ischemia < 0.5%
- Radial nerve injury — zero tolerance
- Optimal damping at 24 h ≥ 85%
- CRBSI < 1 / 1,000 catheter-days
- Documentation completeness 100%
- 01Brzezinski M, Luisetti T, London MJ. Radial artery cannulation: a comprehensive review of recent anatomic and physiologic investigations. Anesth Analg. 2009;109(6):1763–81. PMID 19923502.
- 02Shiloh AL, Savel RH, Paulin LM, Eisen LA. Ultrasound-guided catheterization of the radial artery: a systematic review and meta-analysis. Chest. 2011;139(3):524–9. PMID 20724734.
- 03Scheer B, Perel A, Pfeiffer UJ. Clinical review: complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring. Crit Care. 2002;6(3):199–204. PMID 12133178.
- 04Mariano-Gomes PM, Ouverney-Braz A, Oroski-Paes G. Adverse events with arterial catheters in intensive care units: a scoping review. Enferm Intensiva (Engl Ed). 2024;35(4):410–427. PMID 39004562.
- 05Kopp SL, Horlocker TT, Vandermeulen E, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine evidence-based guidelines (5th ed). Reg Anesth Pain Med. 2025. PMID 39880411.
- 06O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162–e193. PMID 21460264.
- 07The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 07aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 07bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 07cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 07dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 07eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 07fThe Joint Commission. NPSG.06.01.01 — clinical alarm safety; clinically appropriate settings, authority to change parameters, monitoring/response, and periodic accuracy checks for high-risk alarms. National Patient Safety Goals (HAP); effective January 2025.
- 07gThe Joint Commission. NPSG.02.03.01 EP 1 — report critical results of tests and diagnostic procedures within an established time frame; written procedures define which results are critical and to/from whom they are reported. National Patient Safety Goals (HAP); effective January 2025.
- 08The Joint Commission. IC.02.02.01 — implement evidence-based practices to prevent HAIs. 2024.
- 09The Joint Commission. HR.01.06.01 — competence verified before patient care. 2024.
- 10The Joint Commission. MS.08.01.01 / MS.08.01.03 — FPPE and OPPE for privileged practitioners. 2024.
- 11Bress AP, Anderson TS, Flack JM, et al. The management of elevated blood pressure in the acute care setting: a scientific statement from the American Heart Association. Hypertension. 2024;81(8):e94–e106. PMID 38804130.
- 12Wu G, Chen C, Gu X, et al. Ultrasound-Guided Dynamic Needle-Tip Positioning Method Is Superior to Conventional Palpation and Ultrasound Method in Arterial Catheterization: a systematic review and meta-analysis. J Clin Med. 2022;11(21):6539. PMID 36362767.
- 13UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.