Occipital Nerve
Block.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/06_Occipital_Nerve_Block
- In-clinic, low-risk procedure with strong evidence for transformed migraine, occipital neuralgia, and cervicogenic headache.
- Procedural relief routinely outlasts the anesthetic — central modulation of the trigemino-cervical complex drives weeks of benefit.
- GON block reduced chronic-migraine days vs. placebo in a randomized, placebo-controlled trial (Inan 2017).
- Owning this skill keeps headache patients out of the ED and shortens time-to-relief.
Tobin J, Flitman S. Headache. 2009;49(10):1521–33 · PMID 19674126
Anatomy & landmarks.
Describe GON course from C2 dorsal ramus and identify EOP, mastoid, and occipital-artery landmarks on the superior nuchal line.
Indications & contraindications.
Apply accepted indications (occipital neuralgia, cervicogenic, chronic migraine, cluster) and absolute vs. relative contraindications.
Bony-backstop technique.
Execute perpendicular needle insertion to occipital bone, withdraw 1–2 mm, and inject medial to the occipital artery.
Mandatory aspiration.
Aspirate in two planes before every injection — the single highest-yield safety step for LAST prevention.
Consent & time-out.
Lead a TJC UP.01.03.01 time-out confirming patient, procedure, laterality, agent, and dose.
Complication escalation.
Recognize vasovagal, hematoma, and LAST signs; activate the ASRA LAST protocol with lipid emulsion as indicated.
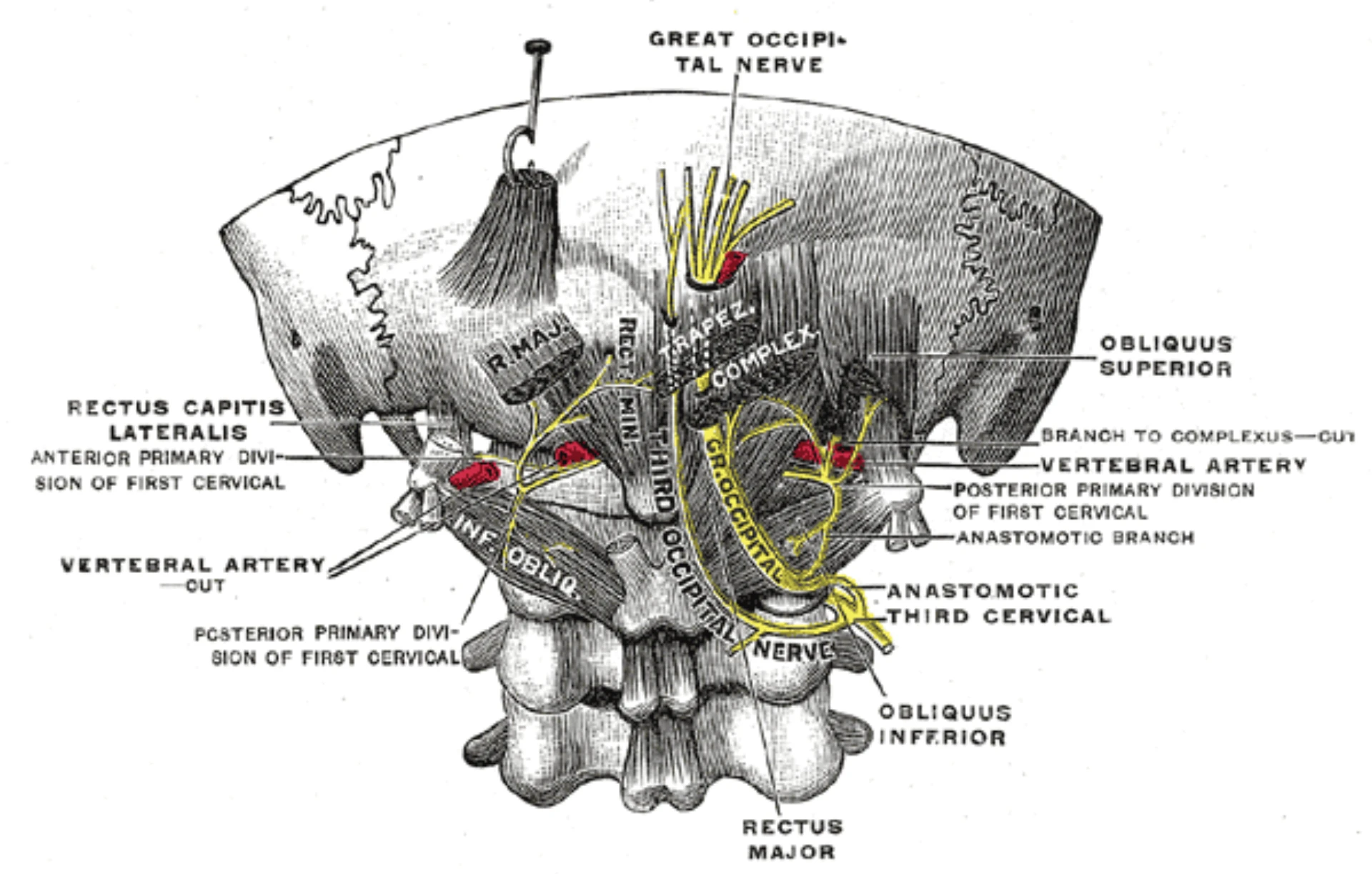
- Arises from the C2 dorsal ramus; pierces semispinalis capitis, then trapezius fascia.
- Emerges subcutaneously over the occipital bone along the superior nuchal line.
- Textbook landmark: ~1/3 of the EOP-to-mastoid distance from the EOP (≈2.5 cm lateral) for the GON entry (Tobin 2009).
- The occipital artery sits adjacent and lateral — the most reliable surface landmark when palpable.
- We aim medial to the artery, perpendicular to the skull, advancing to the bony backstop.
External occipital protuberance.
- Midline bump at the base of the skull
- Anchors the medial end of the superior nuchal line
- Confirms patient is in correct neck flexion
Mastoid process.
- Bony prominence posterior to the ear
- Anchors the lateral end of the nuchal line
- EOP–mastoid line is the working axis
Occipital artery.
- Palpable pulse, lateral to GON
- Mark the artery — enter just medial to it
- LON sits at the ~2/3 mark, posterior border of SCM
- Occipital neuralgia — sharp, paroxysmal, dermatomal pain in the GON/LON distribution; diagnostic + therapeutic.
- Cervicogenic headache — unilateral pain referred from upper cervical structures, reproducible by occipital palpation.
- Chronic migraine / transformed migraine — adjunct to oral or injectable preventives (Blumenfeld consensus; Inan RCT).
- Cluster headache — acute attack and short-term prophylaxis.
- Post-craniotomy / post-traumatic occipital pain and post-concussion headache.
GON block elevated to 'must offer' parenteral therapy for adult ED migraine per the American Headache Society 2025 systematic review — the strongest evidence-grade endorsement of GONB to date.
Blumenfeld A et al. Headache. 2013;53(3):437–46 · PMID 23406160
Gul HL et al. Acta Neurol Scand. 2017;136(2):138–144 · PMID 27910088
- Known allergy to the intended local anesthetic or corticosteroid
- Overlying skin or scalp infection at the planned injection site
- Patient refusal after informed consent
- Therapeutic anticoagulation — apply ASRA Pain Medicine 5th-ed principles; superficial scalp block on a compressible surface tolerates lower thresholds than neuraxial procedures.
- Prior craniectomy with absent occipital bone — loss of the bony backstop dramatically increases the risk of intracranial / vascular injection.
- Pregnancy — block generally safe; minimize steroid exposure.
- Bleeding diathesis — risk–benefit balance.
- 01Informed consent. Indication, alternatives, risks — vasovagal, bruising, intravascular injection, alopecia / fat atrophy from steroid, LAST signs, no guarantee of relief, rebound at 6–8 h, option to decline.
- 02Allergy & med review. Local anesthetic, corticosteroid, latex. Review anticoagulation; ASA / NSAID hold not required.
- 03Laterality decided. Unilateral vs. bilateral; mark the side(s) to be blocked.
- 04Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, site / side, injectate & volume, consent confirmed aloud.
- 05Landmark verification. Palpate EOP, mastoid, and the occipital-artery pulse on the symptomatic side before prep.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
migraine.
'must offer'.
in the review.
over consensus.
- 25–27 G, 1.5-inch hypodermic needle
- 3 mL syringe
- Non-sterile clean gloves
- 2% CHG / 70% IPA prep
- Sterile skin marker
- 1–2 mL bupivacaine 0.5% (or lidocaine 1–2%) per side
- Optional: methylprednisolone 40 mg/mL · or triamcinolone 10–40 mg
- Cotton gauze · adhesive dressing
- Emesis basin · sharps disposal
- Ammonia ampule (vasovagal)
- Supine recliner / Trendelenburg-capable chair
- Pulse oximetry, manual BP cuff
- 20% lipid emulsion per ASRA LAST protocol — bolus 1.5 mL/kg, infusion 0.25 mL/kg/min
- Code-cart access and a clear path to MD page / emergency response
Neal JM et al. ASRA checklist for LAST: 2020 version. Reg Anesth Pain Med. 2021;46(1):81–82 · PMID 33148630
Position ·
seated or prone.
- Seated, leaning forward, forehead on folded arms on a padded bedside table — preferred for cooperative patients
- Alternative: prone with chin tucked, pillow under chest to flex cervical spine
- Part hair along the planned needle track; clip if dense — do not shave
- EOP-to-mastoid line at operator eye level
Landmark ·
EOP · mastoid · artery.
- Palpate EOP and ipsilateral mastoid; draw the imaginary nuchal-line axis
- GON entry ≈ 1/3 of the EOP-to-mastoid distance from the EOP (≈2–3 cm lateral to midline on the superior nuchal line)
- Palpate the occipital-artery pulse · mark the artery · plan to enter just medial to it
- LON, when added, sits at ≈2/3 the EOP–mastoid distance along the posterior border of SCM
Skin prep ·
aseptic no-touch.
- Hand hygiene · non-sterile clean gloves (sterile not required for superficial peripheral block)
- 2% CHG / 70% IPA · friction ≥30 s, dry ≥30 s
- Fenestrated drape; keep syringe, needle, gauze on the field only
- Do not re-palpate the prepped site with ungloved finger — re-mark with sterile marker if needed
Insert to bone ·
aspirate.
- 25–27 G, 1.5-inch needle · perpendicular to skull at the marked entry
- Advance slowly until contact with the occipital bone — the bony backstop
- Withdraw 1–2 mm off periosteum
- Aspirate in two planes — if blood returns, withdraw and re-site before any injectate
- Never inject against resistance or into a paresthesia
Aspirate before every
injection plane.
The occipital artery sits within millimeters of the GON. A 3 mL bolus of bupivacaine into the artery is a LAST event — perioral numbness, metallic taste, tinnitus, then seizure or arrhythmia.
Withdraw. Re-site. Re-aspirate. Inject only when no blood returns in two planes. If a patient reports any LAST prodrome — stop injecting and activate the ASRA LAST checklist.
then 0.25 mL/kg/min infusion.
Neal JM et al. Reg Anesth Pain Med. 2018;43(2):113–23 · PMID 29356773
Slow injection.
- 1.5–3 mL total per nerve site over 20–30 s
- Aspirate before each new plane
- Distribute dose — half at GON, half toward LON when treating both
- Do not inject against resistance
Withdraw + dress.
- Withdraw needle in one smooth motion
- Firm digital pressure 1–2 min over the site
- Massage depot along nuchal line to spread anesthetic
- Adhesive dressing · confirm onset at 5–10 min
Optional LON.
- Add when pain radiates lateral / postauricular
- Target ≈2/3 of EOP–mastoid line, posterior SCM
- Subcutaneous (not to bone) · fan 1–2 mL
- Keep total methylprednisolone ≤ 80 mg/session
Vasovagal.
Most common acute event. Lay supine, ammonia ampule, monitor. Observe ≥15 min seated post-injection.
Arterial puncture · hematoma.
Blood on aspiration → withdraw, re-site. Firm digital pressure 1–2 min to tamponade.
LAST.
Perioral numbness, metallic taste, tinnitus, diplopia → seizure / arrhythmia. Stop · ASRA LAST checklist · 20% lipid emulsion.
Vertebral artery injection.
If needle placed too medial / too deep without bony backstop. Immediate neurosurgery / neurocritical care consult; CT angiography.
Alopecia · fat atrophy.
Focal hair loss or dermal/subcutaneous atrophy at steroid site. Dose-dependent; counsel; space sessions ≥12 weeks.
Rebound headache.
Expected at 6–8 h as lidocaine wears off before steroid takes effect. Counsel up front.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of ON Block privilege | First 3 independent blocks · concurrent review within 14 days · aggregate review at 3-case completion · closed within 6 months |
| OPPE | Continuous baseline · TJC MS.08.01.03 | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication flag |
| Reinstatement | < 5 blocks over 24 mo | Stream B skills checklist re-run + 1 proctored live case |
| Renewal | Biennial · 22 CCR §70703 (CA) | OPPE indicators aggregate · Chair sign-off |
- Vasovagal events requiring rapid-response activation — zero
- LAST events (prodrome or full) — zero
- Aspiration-before-injection documented per laterality — 100%
- Time-out documented including laterality — 100%
- Documentation completeness (consent, agent, volume, technique, tolerance, observation, counseling) — 100%
- 01Tobin J, Flitman S. Occipital nerve blocks: when and what to inject? Headache. 2009;49(10):1521–1533. PMID 19674126.
- 02Blumenfeld A, Ashkenazi A, Napchan U, et al. Expert consensus recommendations for the performance of peripheral nerve blocks for headaches — a narrative review. Headache. 2013;53(3):437–446. PMID 23406160.
- 03Gul HL, Ozon AO, Karadas O, Koc G, Inan LE. The efficacy of greater occipital nerve blockade in chronic migraine: a placebo-controlled study. Acta Neurol Scand. 2017;136(2):138–144. PMID 27910088.
- 04Kissoon NR, Watson JC, Boes CJ, et al. Comparative effectiveness of landmark-guided greater occipital nerve (GON) block at the superior nuchal line versus ultrasound-guided GON block at the level of C2. Clin J Pain. 2022;38(4):271–278. PMID 35132029.
- 05Robblee J, Buse DC, Halker Singh RB, et al. AHS 2025 evidence assessment of parenteral pharmacotherapies for adult emergency-department migraine — greater occipital nerve block Level A 'must offer'. Headache. 2026;66(1):53–76. PMID 41321235.
- 06Kopp SL, Vandermeulen E, McBane RD, et al. ASRA Pain Medicine consensus practice guidelines on regional anesthesia in patients receiving antithrombotic or thrombolytic therapy: 5th edition. Reg Anesth Pain Med. 2025. PMID 39880411.
- 07Neal JM, Barrington MJ, Fettiplace MR, et al. The Third American Society of Regional Anesthesia and Pain Medicine Practice Advisory on Local Anesthetic Systemic Toxicity: Executive Summary 2017. Reg Anesth Pain Med. 2018;43(2):113–123. PMID 29356773.
- 08Neal JM, Neal EJ, Weinberg GL. American Society of Regional Anesthesia and Pain Medicine local anesthetic systemic toxicity checklist: 2020 version. Reg Anesth Pain Med. 2021;46(1):81–82. PMID 33148630.
- 09The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 09aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 09bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 09cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 09dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 09eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 10The Joint Commission. MS.08.01.01 and MS.08.01.03 — Focused and ongoing professional practice evaluation. TJC Hospital Accreditation Standards; 2024.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.