Sphenopalatine Ganglion
Block.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_SPG_Block_Learning_Objectives.docx
- Parasympathetic, sympathetic, and trigeminal pathways converge at the SPG — a single bedside target for multiple primary headaches.
- RCT signal in chronic migraine: repetitive Tx360 block reduced headache intensity vs. saline at 6 months (Cady 2015).
- Cluster headache — acute abortive and short-term prophylaxis during cluster periods (Robbins 2016).
- Acute ED migraine evidence is evolving — Schaffer 2015 saline-vs-lidocaine showed no benefit; McCarthy 2026 dose-finding bupivacaine RCT signals reassessment. Best established evidence remains chronic / cluster.
Cady RK et al. Headache. 2015;55(1):101–16 · PMID 25338927
McCarthy D et al. Ann Emerg Med. 2026 Jan 27 (online ahead of print) · PMID 41603837
Anatomy & indications.
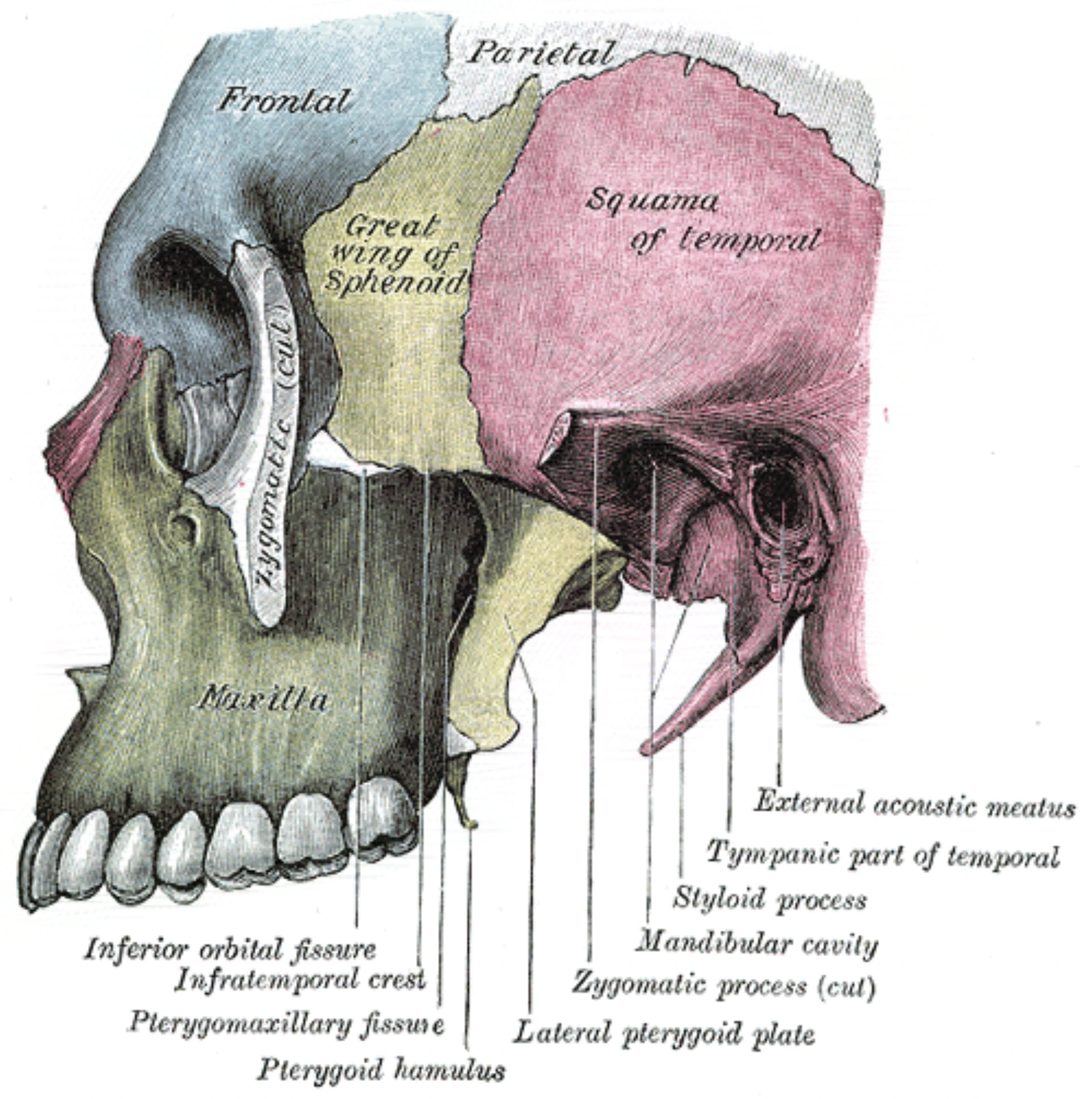
Identify the SPG within the pterygopalatine fossa; state accepted indications and absolute / relative contraindications.
Transnasal corridor.
Position the patient and advance the catheter along the nasal floor to the posterior nasopharyngeal wall — no force, pressure-not-pain.
Anesthetic delivery.
Verify concentration, calculate per-side and cumulative dose against ASRA LAST ceiling, instill slowly, hold the 10-minute dwell.
Complication recognition.
Recognize epistaxis, vasovagal, and the LAST prodrome (perioral numbness, tinnitus, metallic taste). Escalate appropriately.
Time-out & consent.
Lead the team-based time-out per TJC UP.01.03.01 — patient, procedure, laterality plan, anesthetic agent + concentration + volume.
Documentation & escalation.
Document pre / post NRS, device, dose, dwell, complications, disposition. Escalate per pathway when relief fails or complications occur.
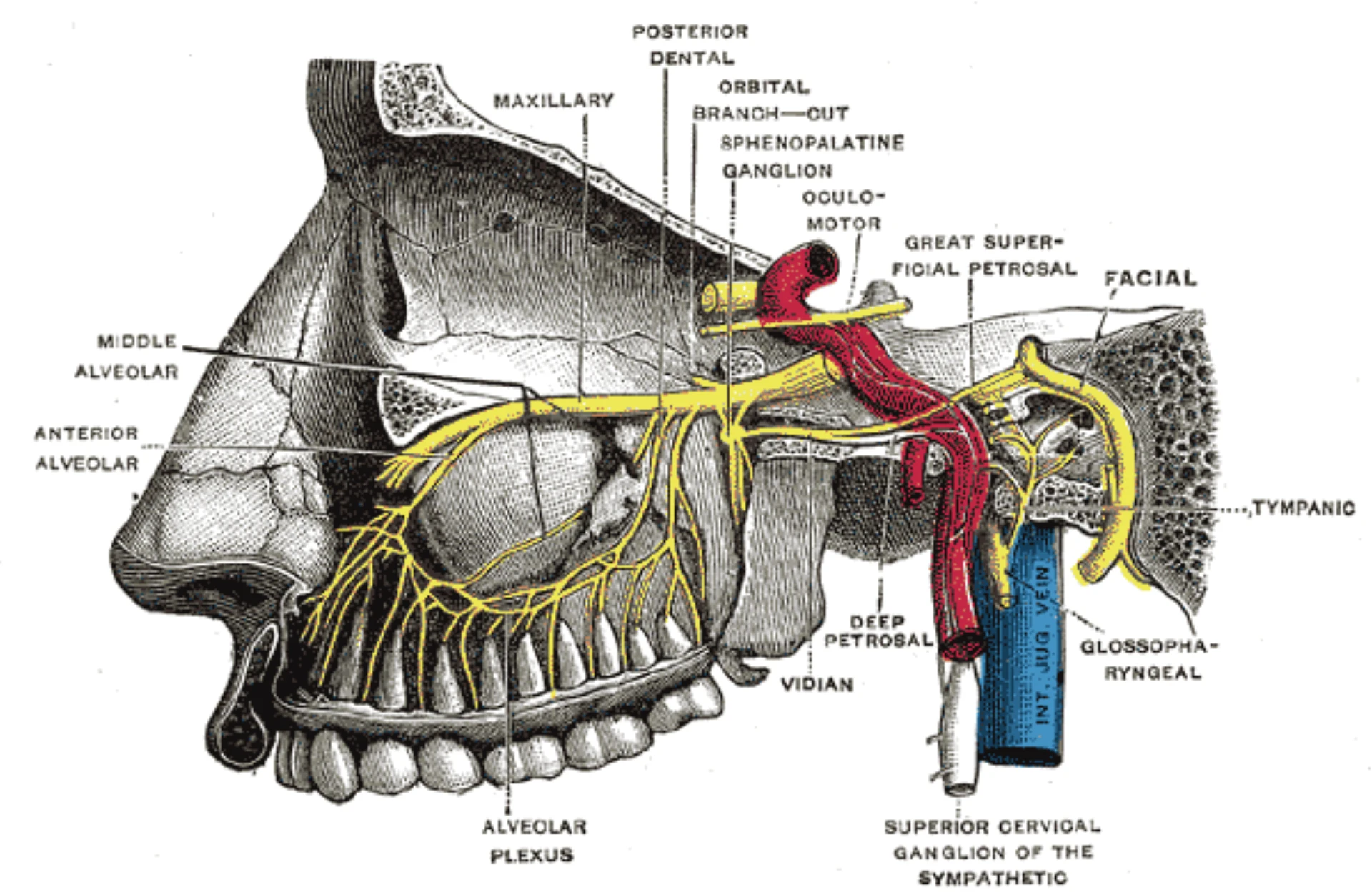
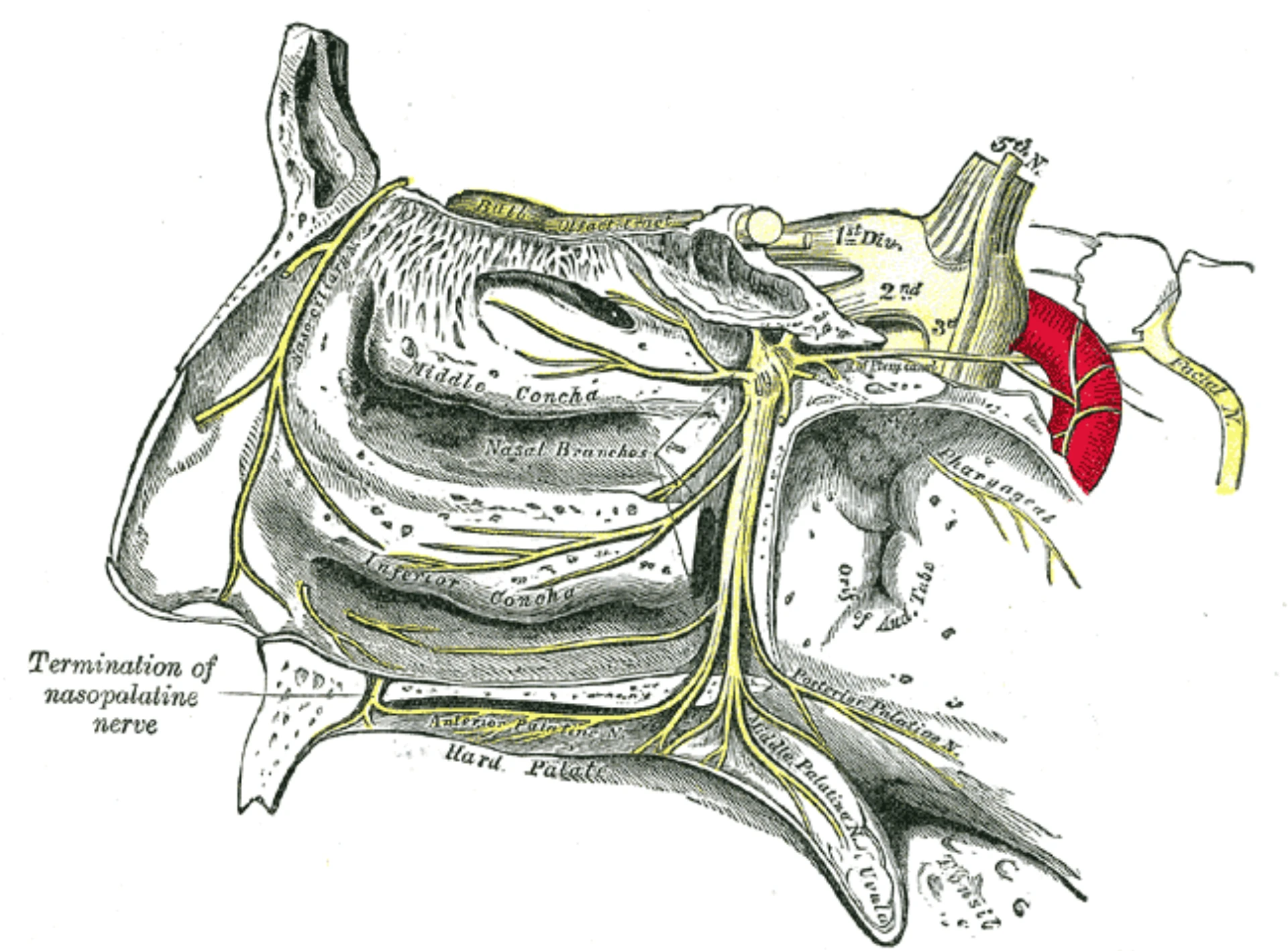
- SPG sits in the pterygopalatine fossa, posterior to the middle turbinate.
- Largest extracranial parasympathetic ganglion — trigeminal sensory and sympathetic fibers converge here.
- Separated from the nasal cavity by 1–1.5 mm of mucosa — accessible to topical anesthetic without injection.
- Parasympathetic outflow drives lacrimation, rhinorrhea, and the cranial autonomic features of cluster and migraine.
Robbins MS et al. Headache. 2016;56(2):240–58 · PMID 26615983
- Trajectory: along the nasal floor, parallel to the hard palate — not angled upward.
- Catheter tip advances past the middle turbinate to rest against the posterior nasopharyngeal wall.
- Mucosal diffusion delivers anesthetic across the lateral nasal wall to the SPG.
- Depth marker on Tx360 / SphenoCath confirms posterior placement (≈ 6 cm in most adults).
- External length should match the pre-measured tragus-to-nostril distance.
- Chronic migraine — adjunct to oral preventives; strongest RCT evidence with repetitive Tx360 protocol.
- Cluster headache — acute abortive and short-term prophylaxis during cluster periods.
- Trigeminal autonomic cephalalgias (paroxysmal hemicrania, SUNCT) — adjunct when oral therapy partial.
- Refractory persistent headache after lumbar puncture or post-traumatic — case-series support; reasonable trial when conservative measures fail.
Robbins MS et al. Headache. 2016;56(2):240–58 · PMID 26615983
- Absolute: active epistaxis · coagulopathy with high bleeding risk
- Absolute: severe septal deviation · recent nasal surgery · sinonasal trauma blocking the corridor
- Absolute: documented amide-LA allergy (lidocaine, bupivacaine)
- Absolute: active sinonasal infection · nasopharyngeal mass · pediatric without specific protocol
- Relative: mild septal deviation · anticoagulation amenable to brief hold · inability to tolerate supine + head extension · uncontrolled allergic rhinitis
- 01Indication confirmed. Accepted indication present; secondary-headache red flags screened out on focused history and exam.
- 02Allergy & contraindications. No amide-LA allergy. No active epistaxis, infection, recent nasal surgery, or sinonasal mass blocking the corridor.
- 03Consent documented. Material risks (epistaxis, dysgeusia, vasovagal, rare LAST, failed relief), alternatives, right to decline — teach-back confirmed before the procedure begins.
- 04Baseline NRS captured. Pre-block headache severity 0–10, side(s) involved, documented.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, laterality plan, anesthetic agent + concentration + volume, consent confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
(20–30 s).
(10–15 min).
at 15 + 30 min.
- Delivery device — Tx360, SphenoCath, MiRx
- Or cotton-tipped applicator (DIY fallback)
- 3 mL syringe · Luer fit verified
- Sterile saline flush
- Gauze · emesis basin
- Non-sterile gloves · mask · eye protection
- Non-sterile drape
- NRS scale (0–10) at bedside
- BP cuff & pulse oximeter for vasovagal screen
- Lipid emulsion 20% available (LAST kit)
- Primary: 4% lidocaine — most common in published transnasal SPG protocols
- Alternative: 0.5% bupivacaine — longer duration when prolonged effect is desired
- Small-volume topical application to the posterior middle turbinate / sphenopalatine recess mucosa
- Bilateral cumulative dose shares the ASRA LAST weight-based ceiling — recalculate per patient
- Verify concentration on the vial — not what you think it should be
- Supine, head extended 20–30° — chin slightly elevated, not hyperextended.
- Goal: align the nasal floor with the posterior nasopharyngeal target plane.
- Older textbooks citing 45° are outdated — Tx360 / Cady 2015 protocol is 20–30°.
- Tilt the head ~10° toward the side being treated to pool anesthetic against the SPG mucosa.
- Position emesis basin and gauze within reach before catheter advancement.
Device prep ·
prime & verify.
- Inspect catheter for kinks · verify hub-to-tip integrity
- Draw anesthetic · verify concentration on the vial
- Attach syringe · prime with 0.5 mL to clear lumen air
- Confirm flow at the tip before nasal insertion
Insert along the
nasal floor.
- Parallel to the hard palate · not angled upward
- Advance steadily until depth marker reaches the naris
- ≈ 6 cm in most adults
- Tip rests at posterior nasopharyngeal wall, past the middle turbinate
Pressure ·
not pain.
- Pressure / fullness = correct trajectory
- Sharp pain = malposition · turbinate contact / false track
- Withdraw 1–2 cm · redirect along the floor · re-advance
- Never force a tight catheter
Pressure — not pain.
Confirm before you instill.
- Patient reports pressure or fullness — not sharp pain
- Catheter depth marker aligns with the nostril rim
- External length matches pre-measured tragus-to-nostril distance
- Patient breathes through the mouth — confirms tip is below the airway plane
- Withdraw 1–2 cm
- Redirect along the nasal floor
- Re-advance with the same pressure / pain feedback loop
- Never force advancement against a tight catheter
Redirect — or abort.
Robbins MS et al. Headache. 2016;56(2):240–58 · PMID 26615983
Slow instillation ·
20–30 seconds.
- Inject 0.5–1 mL over 20–30 s — slow rate limits posterior runoff
- Warn patient: bitter / salty taste is expected
- Lacrimation & mild rhinorrhea = parasympathetic engagement, not adverse
- Stop & reassess on cough, severe gag, or vasovagal symptoms
Hold the dwell ·
withdraw slowly.
- Maintain 10-minute indwelling dwell per side
- Withdraw along the same trajectory used for insertion
- Rapid withdrawal triggers sneeze reflex · aerosolizes anesthetic
- Inspect tip for integrity · gauze ready for blood-tinged discharge
Contralateral ·
fresh catheter.
- Bilateral default for migraine & cluster — unilateral only when strictly one-sided
- Fresh catheter on the second side
- Same anesthetic dose · cumulative against LAST ceiling
- Document side, dose, time for each block separately
- Keep patient supine for 30 minutes to maximize mucosal contact time
- Reassess NRS at 15 and 30 minutes post-block
- Monitor for vasovagal response, persistent epistaxis, new neurologic symptoms
- Screen for early LAST: perioral numbness, tinnitus, metallic taste, agitation
- Tolerance of oral intake before discharge
- Stable vital signs · ambulating without orthostasis
- Headache reduction or stable (partial response acceptable; document)
- Oral intake tolerated
- No active epistaxis · no LAST prodrome
- Return precautions reviewed · headache-clinic follow-up arranged if appropriate
Bitter / salty taste.
Posterior pharyngeal runoff. Warn the patient up front. Resolves within minutes of withdrawal.
Lacrimation & rhinorrhea.
Parasympathetic engagement on the blocked side — a feature, not a bug. Confirms physiologic effect.
Vasovagal.
Pale, diaphoretic, near-syncope, bradycardia. Place supine, legs elevated, IV fluids if symptomatic. Pause; resume only when fully recovered.
Mild epistaxis.
Usually self-limited; gentle alar pressure. Persistent or recurrent bleeding requires ENT consult — most common complication overall.
Posterior pharyngeal numbness.
Transient anesthetic effect on swallow. Hold PO until sensation returns. Reassuring; not LAST.
Cough / gag reflex.
Anesthetic runoff to the airway. Stop instillation, sit patient up, suction if needed. Usually self-limited.
Allergic reaction.
Amide-LA allergy is rare but possible. Standard anaphylaxis algorithm — epinephrine, airway, IV access.
LAST.
Perioral numbness, tinnitus, metallic taste → agitation → seizure → cardiovascular collapse. ASRA LAST protocol · 20% lipid emulsion.
| Agent | mg/kg | Adult max |
|---|---|---|
| Lidocaine (plain) | 4.5 | 300 mg |
| Lidocaine + epi | 7 | 500 mg |
| Bupivacaine | 2 | 175 mg |
- Wrong trajectory: angling the catheter upward toward the cribriform instead of along the floor. Parallel to the hard palate, not pointing at the eye.
- Rushing the dwell: <10 min contact time, then declaring the block ineffective. The block is the dwell.
- Bilateral dose stacking: calculating each side independently against the LAST ceiling. Cumulative bilateral dose shares the same maximum.
- Skipping the time-out / baseline NRS: no documented baseline = no demonstrable response; no time-out = no defense.
| Stage | Scope |
|---|---|
| FPPE | First 5 independent cases after Board approval · concurrent per-case review within 14 days · aggregate at 5 · target close in 6 mo |
| OPPE | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication flag |
| Lapse | < 3 SPG blocks over 24 mo → simulation + 1 proctored case to reinstate |
- Bilateral completion (or documented rationale) 100%
- Epistaxis rate ≤ 10% rolling 6-mo
- Documentation completeness 100%
- Post-procedure observation compliance ≥ 95%
- Severe complication — 100% per-case review
- 01Robbins MS, Robertson CE, Kaplan E, et al. The sphenopalatine ganglion: anatomy, pathophysiology, and therapeutic targeting in headache. Headache. 2016;56(2):240–58. PMID 26615983.
- 02Cady RK, Saper J, Dexter K, Manley HR. A double-blind, placebo-controlled study of repetitive transnasal SPG blockade with Tx360 as acute treatment for chronic migraine. Headache. 2015;55(1):101–16. PMID 25338927.
- 03Schaffer JT, Hunter BR, Ball KM, Weaver CS. Noninvasive sphenopalatine ganglion block for acute headache in the ED: a randomized placebo-controlled trial. Ann Emerg Med. 2015;65(5):503–10. PMID 25577713.
- 04Maizels M, Scott B, Cohen W, Chen W. Intranasal lidocaine for treatment of migraine: a randomized, double-blind, controlled trial. JAMA. 1996;276(4):319–21. PMID 8656545.
- 05Piagkou M, Demesticha T, Troupis T, et al. The pterygopalatine ganglion and its role in various pain syndromes: from anatomy to clinical practice. Pain Pract. 2012;12(5):399–412. PMID 21956040.
- 06Neal JM, Neal EJ, Weinberg GL. ASRA Local Anesthetic Systemic Toxicity Checklist: 2020 Version. Reg Anesth Pain Med. 2021;46(1):81–82. PMID 33148630.
- 07McCarthy D, Borrayes L, Hopper E, et al. A randomized, dose-finding study of sphenopalatine ganglion block with bupivacaine for emergency department patients with headache. Ann Emerg Med. 2026 Jan 27 (online ahead of print). PMID 41603837.
- 08The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 08aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 08bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 08cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 08dThe Joint Commission. Universal Protocol UP.01.02.01 EP 5 — written alternative process for site marking when anatomy precludes a mark (mucosal surfaces, perineum, premature infants, teeth, minimal-access procedures treating a lateralized internal organ). Documented per hospital policy. National Patient Safety Goals (HAP); effective January 2025.
- 08eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 09The Joint Commission. HR.01.06.01 — competence verified before care; MS.08.01.01 / MS.08.01.03 — FPPE / OPPE. 2024.
- 10CDC. Guideline for Hand Hygiene in Health-Care Settings. MMWR. 2002;51(RR-16):1–44.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.