Wound
Suturing.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Suturing_Learning_Objectives.docx
- Decision architecture matters more than knot mechanics — the triage in the first 90 s determines whether you close or refer.
- Three principal hazards drive the FPPE design: missed deep-structure injury, LAST from lidocaine overdose, epi at a forbidden site.
- Wound-outcome OPPE indicators tracked at ≤5% infection, ≤3% dehiscence, ≤5% return-to-ED.
- LAST events tolerated at zero — a single prodrome triggers mandatory focused review of the index case plus 3 subsequent closures.
StatPearls NBK470598 · Wound Closure Techniques
Triage & scope.
List the golden-period windows (face ≤6 h, trunk ≤12 h, scalp ≤24 h); distinguish wounds within APP scope from those requiring referral.
Deep-structure screen.
Examine distal pulse, capillary refill, tendon ROM against resistance, two-point discrimination, joint capsule integrity — refer on any positive.
Lidocaine & LAST math.
Calculate the maximum dose — 4.5 mg/kg plain, 7 mg/kg with epi; identify the epi-forbidden sites: fingers, toes, ears, nose, penis.
Closure technique.
Execute simple interrupted, running, and vertical / horizontal mattress sutures with eversion, equal bite, and knots laid to the side of the wound.
Scalp stapling.
Clip (not shave) hair, approximate edges with Adson forceps, fire staples perpendicular at 5–7 mm spacing without strangulating tissue.
Time-out & escalation.
Lead a TJC UP.01.03.01 time-out with calculated dose and allergy check; activate the ASRA LAST protocol on any prodrome.
| Screen | What you do | Disposition |
|---|---|---|
| Mechanism & time | Date the injury; assess contamination level (clean / contaminated / grossly contaminated); ask about retained foreign material (glass, gravel, soil). | Within golden period — proceed; over window — delayed primary or secondary intention; gross contamination — irrigate, pack, close at 3–5 d. |
| Size · depth | Measure length in cm; probe depth; describe wound bed and edges (clean-edged vs ragged / stellate). | Ragged or stellate edges → conservative debridement; depth involving deep fascia → layered closure with absorbable deep layer. |
| Vascular integrity | Distal pulse; capillary refill at the digit / nail bed distal to the wound; brisk vs delayed. | Any deficit — refer: named-vessel involvement is outside APP scope. |
| Deep-structure screen † | Tendon ROM against resistance at the affected site; two-point discrimination distal to the wound; joint capsule integrity; foreign-body imaging if mechanism warrants. | Any positive → refer to ED, Hand Surgery, or Plastic Surgery. Critical action on the Skills Validation Checklist. |
- Simple, clean-edged adult laceration within golden period
- No deep-structure involvement on screen
- No bite mechanism; no gross contamination
- Scalp closure after EVD / lumbar drain removal — most frequent inpatient use case at UCI
- Trunk & extremity simple lacerations
- Uncomplicated facial laceration not crossing landmarks
- Absolute: tendon, nerve, named vessel, or joint capsule involvement
- Absolute: animal or human bites — primary closure raises infection risk
- Absolute: grossly contaminated wound requiring operative debridement — irrigate & pack, delayed primary at 3–5 d
- Refer: vermilion border crossings, eyelid, alar rim, ear cartilage
- Refer: facial lacerations requiring plastic-surgery cosmesis
- Refer: wounds beyond golden period — secondary intention
• Plain: 315 mg ≈ 31 mL
• With epi: 490 mg ≈ 49 mL
nose · penis.
Perioral numbness · tinnitus · metallic taste · diplopia · seizure · arrhythmia. 20% lipid emulsion 1.5 mL/kg bolus, then 0.25 mL/kg/min per ASRA 2020.
- Mayo-Hegar needle driver
- Adson tissue forceps (toothed)
- Iris scissors · suture scissors
- Suture pack matched to site
- Skin stapler (scalp only)
- Sterile drape · sterile gloves
- 1% lidocaine vial + epi vial (separately racked)
- 10 mL syringe · 27 g infiltration needle
- 30–60 mL irrigation syringe
- 18 g angiocath or splash shield
- Sterile saline bottle (≥ 500 mL)
- CHG-alcohol prep · gauze
| Face | 5-0 or 6-0 nylon / polypropylene · simple interrupted |
| Scalp | 3-0 or 4-0 nylon or staples |
| Trunk | 4-0 nylon / polypropylene |
| Extremity | 4-0 or 5-0 nylon |
| Deep layer | 4-0 Vicryl or Monocryl (absorbable) |
- 01Consent documented. Indication, alternatives including referral for out-of-scope wounds, material risks — infection, dehiscence, cosmetic result, keloid, LAST — and the patient's right to decline.
- 02Allergy & tetanus check. Lidocaine · CHG · latex. Td / TdAP status — per CDC, q10 y; q5 y if dirty wound and > 5 y since last booster.
- 03Lidocaine dose calculated. Compute the mg ceiling for the patient's weight BEFORE drawing up; state the mL ceiling for the 1% solution; defer if proposed dose exceeds ceiling.
- 04Epi-forbidden zones verbalized. If any anesthetic is being prepared, state the forbidden-site list aloud as an audible safety pause.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient · procedure · site / laterality · calculated dose · allergy check · consent confirmed aloud.
UP.01.03.01
UCI APP Class 2 Training Plan Process · TJC HR.01.06.01.
Prep ·
sterile field.
- CHG-alcohol — concentric circles, center out
- Allow appropriate dry time, do not blot
- Drape; sterile gloves; tray laid out
- Adequate lighting; ergonomic positioning
- Povidone-iodine if CHG contraindicated
Irrigate ·
volume drives outcome.
- ≥ 50–100 mL sterile saline per cm of wound
- Moderate pressure — splash shield or 18 g angiocath on 30–60 mL syringe
- State volume aloud
- Tap water acceptable if saline unavailable
Infiltrate ·
wait for onset.
- Through wound edges (less painful) — or intact skin if heavily contaminated
- Aspirate before injecting; inject slowly
- Wait 60–90 s for onset before cutting
- Monitor for LAST prodrome continuously — pause on any report
Selective sharp debridement.
- Remove only clearly devitalized or necrotic tissue
- Preserve viable tissue — over-debridement raises tension and worsens cosmesis
- Iris scissors for fine work
- If mechanism suggests retained foreign material — obtain imaging and defer closure pending result
- Address dead space before skin closure — absorbable deep layer if needed
- Monofilament (nylon, polypropylene) — lower infection risk, slides through tissue cleanly
- Braided (silk, Vicryl) — better knot security but harbors bacteria; reserved for deep layers
- Absorbable for deep / buried layers (Vicryl, Monocryl); non-absorbable for skin (removed at the timing window)
- Smaller caliber on cosmetically visible skin — face = 5-0 / 6-0
- Larger caliber on hair-bearing scalp where tension > cosmesis
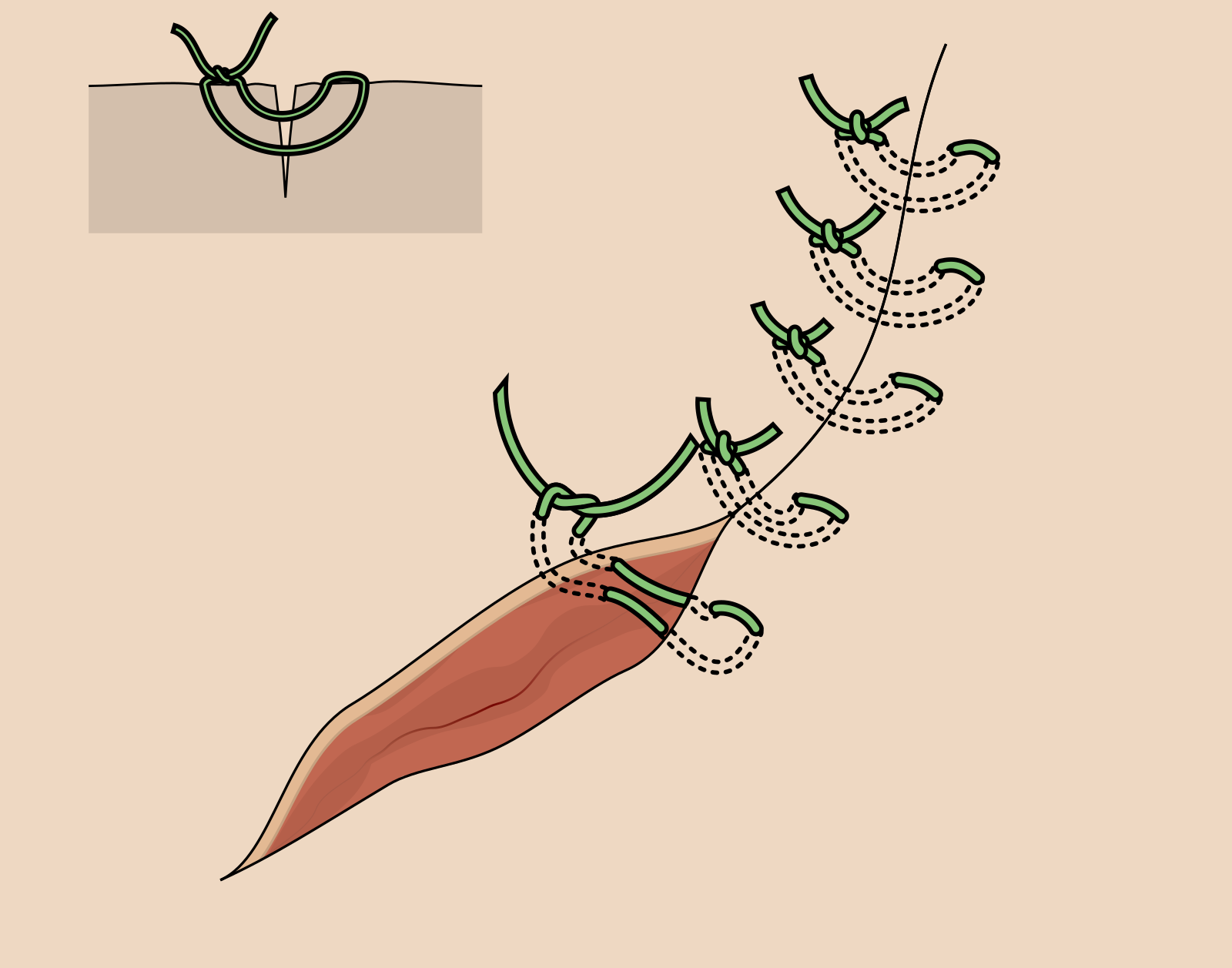
- aPerpendicular entry. Drive the needle through one edge at 90° to the skin; equal bite on both sides; depth equal to width creates eversion.
- bMirror exit. Exit through the opposite edge at the matching depth; pull through smoothly with the needle driver.
- cSurgeon's knot · 2-1-1. Double throw first (holds tension while flat), then single, then single — three throws total for nylon / polypropylene.
- dLay knots to the side. Knots rest off the wound line, not over it — reduces inflammation at the apposition.
- eApproximate, do not strangulate. Snug enough for edges to touch and gently evert; not so tight that tissue blanches.

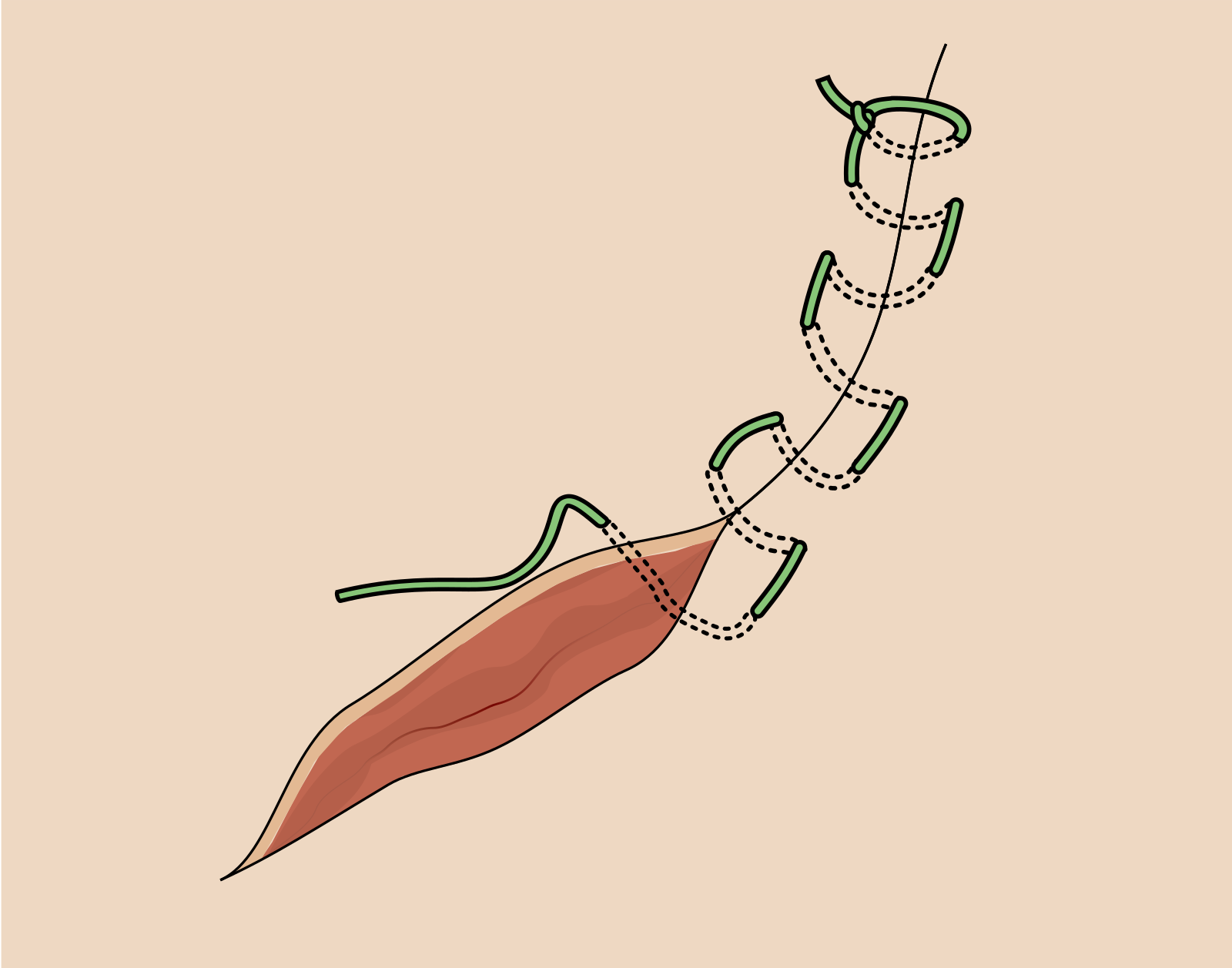
Long · clean · low-tension.
- Anchor with an interrupted knot
- Continuous stitches ~5 mm apart
- Final knot tied to a loop
- Avoid on high-tension, contaminated, or cosmetic facial wounds
- Long trunk & scalp lacerations only
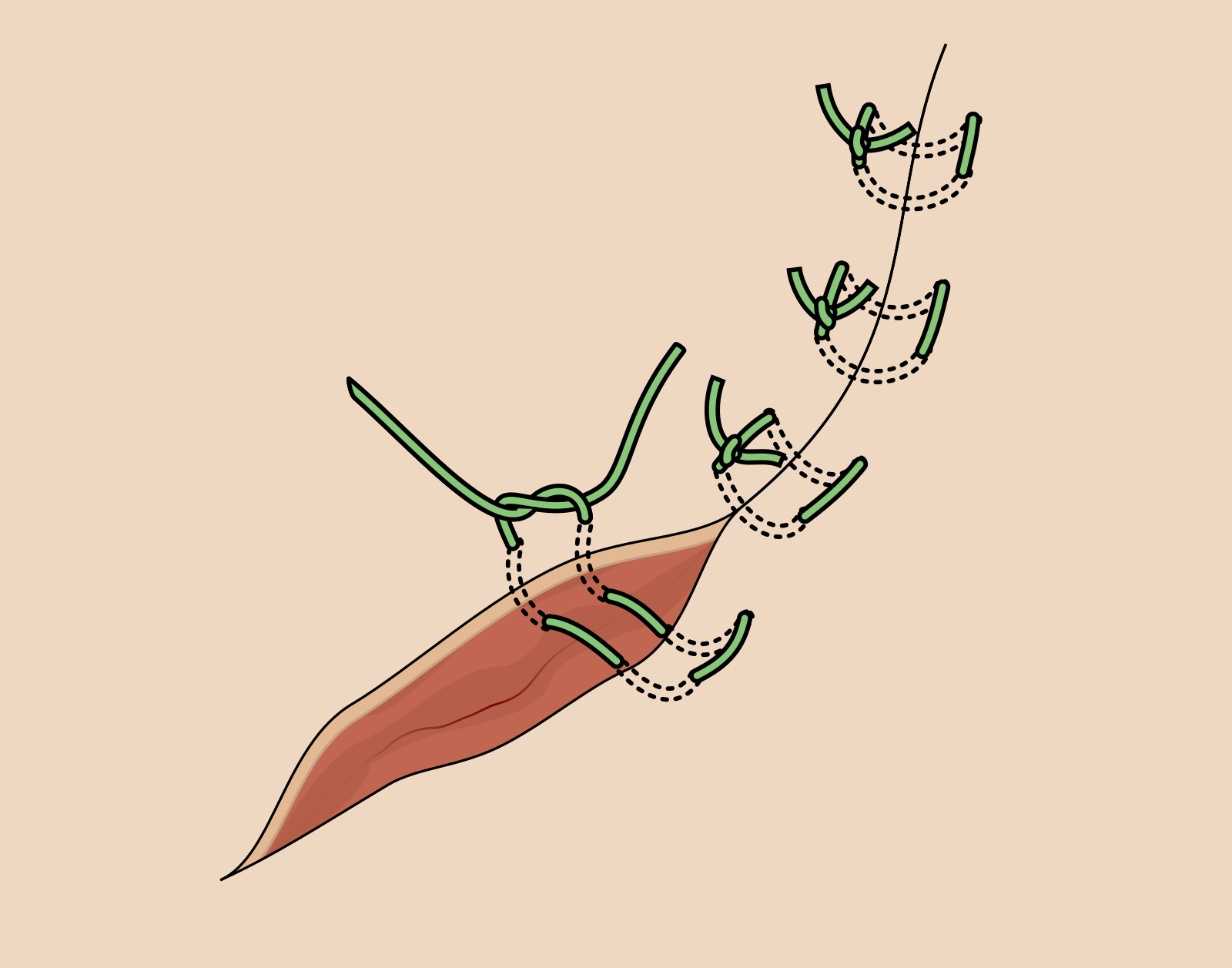
High tension · everts edges.
- Far-far, near-near on the same side
- Distributes tension across two depths
- Forces edge eversion in inverting wounds
- Remove earlier than interrupted to avoid track marks
Thin skin · hemostasis.
- Across the wound, then back parallel
- Spreads tension along the wound line
- Useful for thin atrophic skin
- Hemostatic — compresses bleeding edge
- Same early-removal discipline
- aConfirm scope. Staples are scalp only in APP scope. Wound must be clean-edged, within golden period, no deep-structure involvement, no gross contamination.
- bClip — do not shave. Razor shaving is associated with higher surgical-site infection risk vs clippers — moderate-certainty evidence (Cochrane: Tanner J, Melen K, 2021); Forsch 2017 (AFP) notes shaving is rarely necessary. Bailey 2025 (Eplasty) literature review on scalp-laceration repair supports staples as a hair-sparing closure. Verbalize the rationale.
- cApproximate edges. Adson forceps with teeth; pull edges together without crushing.
- dFire perpendicular. Stapler held perpendicular to the wound line; place at ~5–7 mm spacing; approximate without strangulating tissue.
- eNo ointment under staples. Dressing is gauze or simple non-adherent — no antibiotic ointment under staples.
- Anticoagulated scalp laceration — fewer manipulations near a bleeding edge; faster operator time
- Post-EVD / post-LD exit-site closure on the inpatient ward
- Trade-off: less refined cosmetic appearance, acceptable on hair-bearing scalp
Evert the edge. Remove on time.
Edges that turn outward heal flush. Edges that invert heal depressed. Achieve eversion by perpendicular needle entry, depth equal to width, and gentle tissue handling with toothed Adson forceps.
| Face | 5 days |
| Scalp | 7–10 days |
| Trunk | 7–10 days |
| Extremity | 10–14 days |
| High-tension / joint | 10–14 days + steri-strips after removal |

Infection.
Cellulitis, abscess, or purulent drainage. OPPE ceiling ≤ 5% over rolling 12 mo.
Dehiscence.
Separation at / before scheduled removal. OPPE ceiling ≤ 3%.
Hypertrophic / keloid.
Patient-specific risk — anterior chest, deltoid, earlobe. Counsel pre-procedure.
Suture track marks.
Left too long or tied too tight. Mattress sutures removed earlier than interrupted.
LAST.
Single prodrome triggers mandatory focused review of the index case + 3 subsequent closures. Activate ASRA 2020 protocol; 20% lipid emulsion 1.5 mL/kg bolus then 0.25 mL/kg/min.
- 01Skipping the deep-structure screen. Highest-harm error in the procedure — closes a tendon or nerve laceration beneath an intact-appearing skin closure. Critical action †.
- 02Knots over the wound · tied too tight. Track marks and depressed scar. Lay knots to the side; approximate, do not strangulate.
- 03Running suture on high-tension wound. Dehiscence — running redistributes tension along a single strand; interrupted compartmentalizes failure.
- 04Epi at a forbidden site. Trigger for ad-hoc focused review regardless of patient outcome — fingers, toes, ears, nose, penis: plain lidocaine only.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of suturing / staple privilege | First 3 independent cases · scalp + extremity + face mix where volume allows · within 6 mo |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review of any complication-flagged case |
| Trigger review | LAST · epi-forbidden site · missed deep-structure · I&D-level infection | Index case + next 3 closures reviewed |
| Reinstatement | < 10 closures in rolling 24 mo | Stream B skills checklist + 1 proctored case rated Independent |
| Renewal | Biennial · 22 CCR §70703 (CA) | OPPE indicators aggregate · Chair sign-off |
- Wound infection rate ≤ 5% rolling 12 mo
- Dehiscence rate ≤ 3% rolling 12 mo
- Return-to-ED for wound issue ≤ 5%
- LAST event rate = 0 (single event → focused review)
- Epi-forbidden-site adherence 100%
- Documentation completeness 100%
- 01Forsch RT, Little SH, Williams C. Laceration repair: a practical approach. Am Fam Physician. 2017;95(10):628–636.
- 02Neal JM, Neal EJ, Weinberg GL. ASRA Local Anesthetic Systemic Toxicity Checklist: 2020 Version. Reg Anesth Pain Med. 2021;46(1):81–82.
- 03StatPearls. Wound Closure Techniques. NBK470598. Treasure Island, FL: StatPearls Publishing; updated 2024.
- 04Li L, Shao Q, He W, Wang T, Wang F. Close orthopedic surgery skin incision with combination of barbed sutures and running subcuticular suturing technique for less dermal tension concentration: a finite element analysis. J Orthop Surg Res. 2023;18(1):333. PMID: 37147669 · PMC10163751.
- 05Alijani M, Jamshidi S, Nadripour R, Kamyari N, Heidari A. The use of cyanoacrylate tissue adhesives in various wound suturing techniques to enhance the healing process of surgical wounds: an animal study. Clin Exp Dent Res. 2025;11(1):e70057. PMID: 40052462 · PMC11886599.
- 06Bailey V, Kherallah K, Warner J, Moffit S, Moore M. Mitigating Hair Loss Among Scalp Laceration Repair Techniques: Review of the Literature. Eplasty. 2025;25:e29. PMID: 40661091 · PMC12257963.
- 06aTanner J, Melen K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2021;(8):CD004122. doi:10.1002/14651858.CD004122.pub5 · PMID: 34437723.
- 07The Joint Commission. Universal Protocol UP.01.03.01 — pre-procedure verification, site identification, time-out. TJC Hospital Accreditation Standards; 2024.
- 07aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 07bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 07cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 07dThe Joint Commission. Universal Protocol UP.01.02.01 — mark the procedure site; mark by the accountable licensed practitioner (APRN/PA delegation permitted per institutional policy); unambiguous, visible after prep & drape. National Patient Safety Goals (HAP); effective January 2025.
- 07eThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 08The Joint Commission. HR.01.06.01 — competence verified before care. TJC Hospital Accreditation Standards; 2024.
- 09The Joint Commission. MS.08.01.01 & MS.08.01.03 — FPPE / OPPE for privileged practitioners. TJC Medical Staff Standards; 2024.
- 10California Code of Regulations 16 CCR §1474 (Standardized Procedures, NP) · §1399.541 (PA scope). State of California; current.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.
- 1201_Suturing_Learning_Objectives.docx · v1.0 · 2026-04-23 — Appendix A of the Suturing Training Plan (authoritative objectives + mapping table).
- 1303_Suturing_Competence_Assessment.docx · 22-item Skills Validation Checklist · 4 critical actions (†) — UCI APP Education, 2026.