Suture & Staple
Removal.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_LO · 03_CA · 04_PT · 05_FPPE
reassessment.
- Timing affects scar quality on the face and dehiscence risk at high-tension sites.
- Removed count must equal the original closure-note count — count-match is the safety gate.
- Active infection or mid-wound dehiscence is an absolute contraindication to proceed without supervising-physician input.
- Steri-strip reinforcement on early removal, high-tension wounds, or steroid-thin skin reduces dehiscence at 48–72 h.
Timing by anatomic site.
Face 3–5 d · scalp 7–10 d · extremity 7–14 d · trunk 10–14 d · overlying joints 10–14 d.
Read the wound first.
Distinguish adequate healing (apposed, ≤2 mm halo, dry) from concerning signs that should escalate.
Suture-removal technique.
Lift the knot, cut below at the skin surface, pull through the above-skin side — never drag external segment through tract.
Staple-removal technique.
Both lower tines under staple center, squeeze fully so both arms disengage, lift straight up — never lever sideways.
Count-match completion.
Removed count = closure-note count. Uncertain count? Pull the chart before declaring done.
Escalate before — not after.
Active infection, dehiscence, retained-fragment concern, steroid-thin skin → supervising physician before proceeding.
| Site | Standard window | Why | Reinforcement |
|---|---|---|---|
| Face | 3–5 days | Fast healing; suture-track scarring shows cosmetically — earliest removal window. | Steri-strips 48–72 h if any tension. |
| Scalp | 7–10 days | Often staples; hair makes interrupted sutures awkward. Galea tension moderate. | Optional — site-dependent. |
| Extremity | 7–14 days | Tensile-strength window varies with patient factors and wound tension. | Consider on high-tension or joint-adjacent. |
| Trunk | 10–14 days | Slower epidermal turnover; respiratory tension on closure. | Site-dependent; thin skin → yes. |
| Overlying joint | 10–14 days | Constant mechanical tension on the closure — highest dehiscence risk in this table. | Always — perpendicular strips, 48–72 h. |

- Apposition. Edges still together at every point along the wound — note any gapping.
- Drainage. Dry · serosanguinous · or purulent — purulent halts the procedure.
- Erythema halo. ≤ 2 mm pink halo is normal; > 2 mm or extending erythema escalates.
- Warmth & tenderness. Beyond the expected post-op range — concerning.
- Fluctuance. Palpate gently — fluid collection = do not remove over it.
- Active infection at the wound site with purulent drainage.
- Mid-wound dehiscence > 1–2 mm — supervising physician decision.
- Fresh hematoma or fluctuance over the closure.
- Retained-fragment concern at any point in removal.
- Skin tear / friable skin in elderly or steroid-exposed patients with early healing.
- Wound not yet healed enough for the site's standard window.
- High-tension wound — joint, dorsum of hand, lower extremity in active use.
- Systemic steroids · anti-neoplastic therapy · poorly controlled diabetes.
- Concerning healing trajectory at follow-up — leave in place, reassess in 3–5 d.
- Closure-note count uncertain — pull the chart before starting.
- Adson forceps (toothed)
- Suture scissors (sharp-tip)
- Disposable surgical-staple remover
- Sterile saline OR 2% CHG / 70% IPA
- Gauze 4×4 · cotton-tipped applicators
- Clean gloves (sterile per institutional variant)
- Bedside sharps container
- Steri-Strips (assorted widths)
- Tincture of benzoin (optional adhesive prep)
- Procedural light · clean tray surface

- 01Hand hygiene & field. Establish clean sterile field on the tray; don clean gloves (sterile gloves per institutional variant when indicated). Sharps container at the bedside.
- 02Identify closure type. Simple interrupted · mattress (vertical or horizontal) · staples — select correct tool before opening the kit. (Skills item 7.)
- 03Patient position & lighting. Optimize lighting on the wound; position the patient for the site. Explain the procedure and what to expect in plain language.
- 04Surface cleaning. Sterile saline or chlorhexidine-alcohol over the wound surface; allow appropriate dry time before the first cut.
- 05State the count. Read the original closure-note count out loud — site, closure type, documented number — before the first cut. The low-tier time-out.
"What you'll feel · what I'll do · what I'm watching for."
Skills Validation Checklist · Section 2 — setup & sterile field.
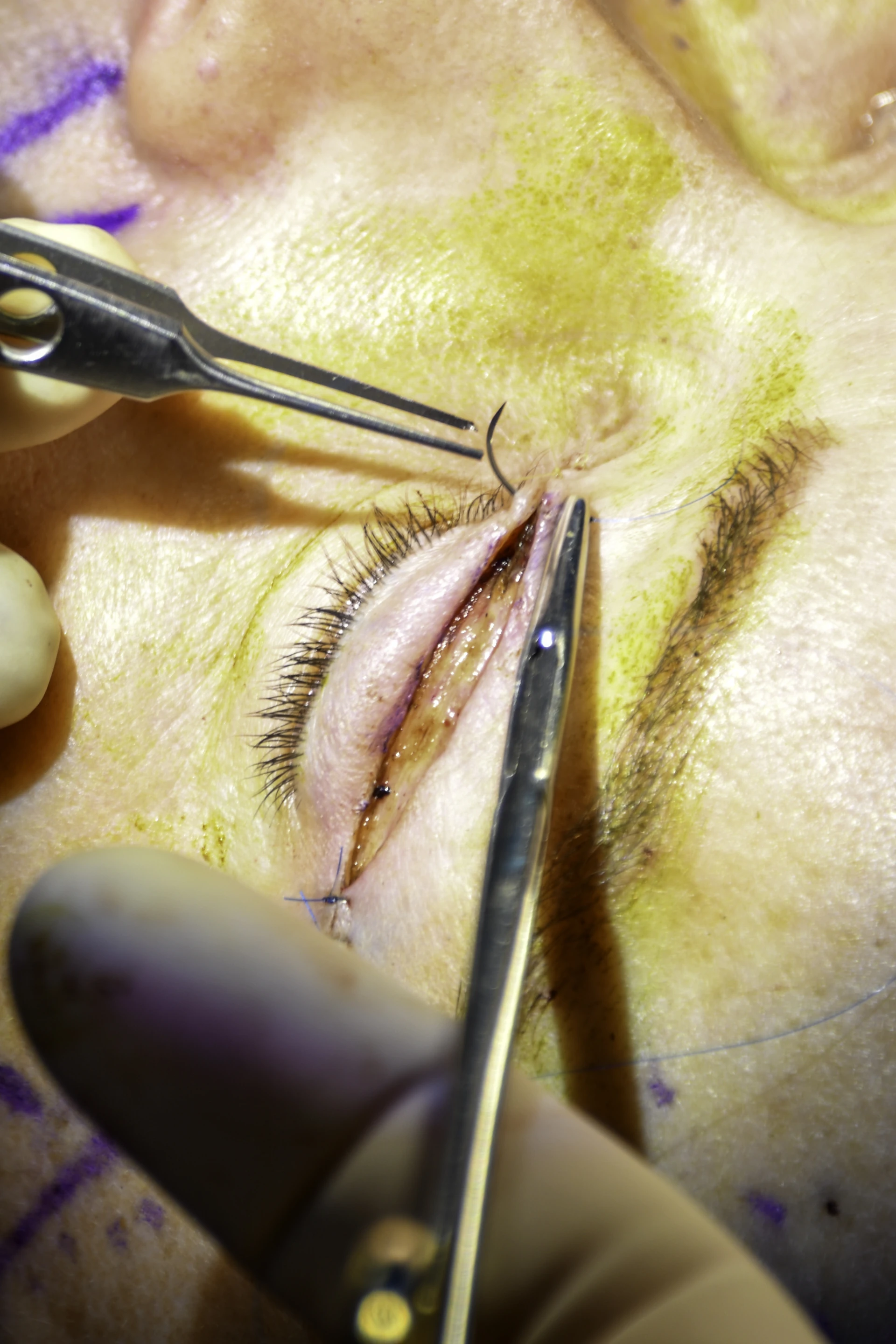
- 01Grasp the knot. Adson forceps · lift gently away from the skin so the suture exit points on each side are visible.
- 02Cut below the knot. At the skin surface — not above the knot, not in the middle.
- 03Pull through the above-skin side. The external segment carries skin flora — never drag it through the subdermal tract.
- 04Inspect & count. Each removed suture intact on inspection · count aloud · drop to gauze square, sharps at end.
- Higher-tension closure pattern — two surface segments per stitch.
- Identify both exposed portions before cutting any.
- Cut both at the skin surface before any segment is withdrawn.
- If you cut and pull on one side without cutting the other, you have just dragged external suture through the deeper bite.
- If the pattern is not identifiable — escalate, do not improvise.
The reason is the same as simple interrupted, multiplied — two external segments means two opportunities to drag skin flora through subdermal tissue if you withdraw before both are cut.
Seat both
lower tines.
- Both lower tines fully under the staple center
- Tool perpendicular to the skin surface
- Confirm seating before squeezing
Squeeze fully —
both arms.
- Squeeze the handles fully · the crown bends
- Both arms disengage simultaneously
- Partial squeeze = partial release = skin tear risk
Lift straight up.
- Perpendicular lift — never lever sideways
- Lateral motion tears the dermal bite
- Drop to sharps · count aloud each staple
Pull toward the wound.
Lift perpendicular to the skin.
Cut below the knot at the skin surface. Pull through the side that was above the skin — toward the wound. The external segment carries skin flora; pulling it through the subdermal tract is how a clean removal becomes a wound infection.
Lift perpendicular to the skin — never lever sideways. Lateral lever motion tears the dermal bite and is a leading cause of dehiscence at the moment of removal — a tracked OPPE indicator.
Escalate before retrying.
UCI APP Class 2 Training Plan Process.
- Removed count = original closure-note count.
- Count uncertain → re-inspect under good lighting, palpate carefully, review the operative note.
- Still uncertain → pull the chart before declaring completion.
- Skills item 13 (critical) · Post-Test Q7 case stem.
- High-tension location · joint · dorsum of hand · trunk under respiratory tension.
- Earlier-than-standard removal.
- Minor edge gapping or steroid-thin skin.
- Perpendicular strips · ~3 mm spacing · leave 48–72 h.
Dehiscence at removal.
Wound opens during or within 24 h. OPPE indicator 3 (monitored trend). Steri-strip; escalate if > 1–2 mm.
Late wound infection.
Erythema, drainage, fever 1–7 d post-removal. Often a contaminated subdermal tract — preventable by the direction rules on slide 14.
Retained fragment.
Suture or staple piece left behind. Return precaution must be given to the patient — palpable bump, drainage, persistent tenderness.
Hypertrophic scar.
Late finding · counseling, not emergency. Sun protection + moisturization after re-epithelialization is the patient-education frame.
Skin tear.
Elderly · steroid-exposed · friable skin. Stop, escalate, reinforce with Steri-Strips perpendicular to the tear axis.
7-day return-to-ED.
Wound complication within 7 d of removal — infection, dehiscence, retained fragment. Target ≤ 1 per 100 removals (monitored).
Cutting above the knot or in the middle.
Pulls the external suture segment through the subdermal tract — direct cause of late wound infection. Always cut below the knot at the skin surface.
Leaving a fragment behind.
Suture breaks mid-removal · staple legs disengage unevenly · count not enforced. Inspect every removed item; if broken, document and escalate.
Premature removal · no reinforcement.
High-tension wound or steroid-thin skin removed at the standard window without Steri-Strips — dehiscence at 24 h. Reinforce when in doubt.
Declaring completion on an uncertain count.
Removed count does not match closure note → pull the chart, re-inspect, palpate. Never document "complete" on a guess.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of removal privilege | First 5 independent removals · per-case review within 30 d · aggregate at 5-case completion · closed within 6 mo |
| OPPE | Continuous baseline · TJC MS.08.01.03 | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication or 7-d return |
| Reinstatement | < 5 cases over 24 mo | 1 proctored live case (not 3) rated Independent · LOW-tier scaling |
| Renewal | Biennial · 22 CCR §70703 (CA) | OPPE indicators aggregate · Chair sign-off |
- Count-match rate 100% (removed = closure-note count)
- Documentation completeness 100% (pre · count · post · aftercare)
- Dehiscence-at-removal — monitored as a trend
- 7-day return-to-ED for wound complication ≤ 1 per 100 removals
- Escalation appropriate on every concerning finding
- Steri-Strip reinforcement applied when indicated
- 01Forsch RT, Little SH, Williams C. Laceration repair: a practical approach. Am Fam Physician. 2017;95(10):628–636. PMID: 28671402.
- 02Richards E, Brown A, Chottianchaiwat S, Frewen J, Powell R, McGrath E. Timing of suture removal to reduce scarring in skin surgery: a randomized assessor-blinded feasibility trial. Clin Exp Dermatol. 2024;49(4):394–397. PMID: 37983174.
- 03Azmat CE, Council M. Wound closure techniques. In: StatPearls. Treasure Island (FL): StatPearls Publishing; last updated 2023 Jun 26. NBK470598.
- 04Niederstätter IM, Schiefer JL, Fuchs PC. Surgical strategies to promote cutaneous healing. Med Sci (Basel). 2021;9(2):45. PMID: 34208722.
- 05UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.
- 06The Joint Commission. HR.01.06.01 — competency assessment of staff. TJC Hospital Accreditation Standards; 2024.
- 07The Joint Commission. MS.08.01.03 — ongoing professional practice evaluation (OPPE). TJC Hospital Accreditation Standards; 2024.
- 07aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 07bThe Joint Commission. Universal Protocol UP.01.03.01 — time-out (applies to all surgical and nonsurgical invasive procedures, including scaled low-tier procedures such as suture/staple removal); team agreement on correct patient, site, procedure; documented. National Patient Safety Goals (HAP); effective January 2025.
- 07cThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 07dThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 08California Code of Regulations. Title 22 §70703 — California 2-yr (biennial) reappointment requirement for acute hospital medical staff. (Per CITATION_AUDIT 2026-04-28: MS.07.01.03 is the TJC disaster-privileging standard, not the biennial-renewal anchor; the controlling cite in CA is 22 CCR §70703. TJC general renewal cycle moved to 3 years in Nov 2022; state law controls when shorter.)
- 09California Code of Regulations. 16 CCR §1474 — Nurse practitioner standardized procedures. Title 16, Division 14.
- 10California Code of Regulations. 16 CCR §1399.541 — Physician assistant scope of practice. Title 16, Division 13.5.
- 11Centers for Medicare & Medicaid Services. Conditions of Participation 42 CFR §482.22 — Medical Staff credentialing and privileging.
- 12UCI Suture/Staple Removal Skills Validation Checklist. 17 items · 4 critical actions (†) · v1.0 · 2026-04-23. Department of Neurology APP Education.
- 13UCI Suture/Staple Removal FPPE/OPPE Plan. LOW-tier scope · 4 indicators · v1.0 · 2026-04-23. Department of Neurology APP Education.