Urinary Catheter
Insertion.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
- The majority of CAUTI episodes trace to catheters placed without a current indication, or left in beyond the indication window.
- Daily indication review with prompt removal is the single highest-yield CAUTI-prevention intervention.
- SHEA Compendium update reaffirms: limit insertion, ensure prompt removal.
- Forced insertion against firm resistance is the dominant mechanism of urethral injury — a preventable, long-tail complication.
Patel PK et al. Infect Control Hosp Epidemiol. 2023;44(8):1209–1231 · PMID 37620117
Indications & anatomy.
Differentiate CDC-accepted indications from inappropriate ones; describe female (~2 in) and male (~8 in, prostatic curve) urethral anatomy.
Catheter selection.
Select straight vs. Foley; 14 Fr standard, 16 Fr hematuria, Coude for BPH; 10 mL balloon inflated with sterile water only.
Sterile technique.
Sterile field, fenestrated drape, meatal prep per institutional policy; catheter remains sterile throughout the advance.
Insertion · female + male.
Midline advance in the female; 90° → 45° two-phase angle in the male; advance to urine return, then 1–2 in further.
Urine return before inflation.
Confirm urine return BEFORE balloon inflation — every time. Inflate with 5–10 mL sterile water.
Escalation & daily review.
Recognize BPH resistance, suspected stricture, blood at meatus — stop, escalate to urology. Daily necessity review & prompt removal.
- Acute urinary retention (bladder scan ≥ 400 mL + symptoms)
- Accurate strict I/O in critically ill / pressor-dependent patients (shock, aSAH, status, TTM)
- Sacral / perineal pressure injury in an incontinent patient — wound healing threatened by urine
- Prolonged immobilization with skin-integrity risk
- Selected peri-operative — anticipated long case, large fluid shifts, anticipated post-op monitoring
- Comfort at end-of-life per patient or surrogate preference
- Substitute for nursing care of an incontinent patient (without wound indication)
- Urine specimen collection in a continent patient
- Routine monitoring of a cooperative, ambulatory patient
- Incontinence alone — without sacral / perineal wound
- Prolonged post-operative use without ongoing need
Hooton TM et al. IDSA. Clin Infect Dis. 2010;50(5):625–63 · PMID 20175247
- Blood at the meatus — most sensitive sign
- Perineal hematoma or "butterfly" ecchymosis
- High-riding or non-palpable prostate on rectal exam (male)
- Pelvic ring fracture with any of the above
- Known urethral stricture history — Coude tip, lidocaine dwell, low threshold to call urology
- Severe BPH or prior difficult male insertion — Coude tip, concave-up
- Recent prostatic, urethral, or pelvic surgery — discuss with surgical team first
- Latex allergy — silicone catheter; iodine allergy — chlorhexidine prep; lidocaine allergy — plain lubricant
- 01Indication verbalized. State the CDC-accepted indication aloud and write it in the procedure note. If you can't name an indication on the accepted list, don't place the catheter.
- 02Consent & alternatives. Discuss risks, alternatives (condom catheter, external female wick / PureWick, straight-cath only), and right to decline. Offer chaperone where appropriate.
- 03Allergy check. Latex · iodine · lidocaine · chlorhexidine. Cross-check kit contents against allergy list before opening.
- 04Patient positioned. Female — supine, frog-leg, draped. Male — supine, legs extended, draped. Light source positioned.
- 05Time-out called. Per TJC UP.01.03.01 — two identifiers, correct procedure, site (urethral vs. suprapubic), indication, allergies confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
at placement.
insertion.
bag below.
review.
removal.
- 14 Fr Foley · standard adult
- 16 Fr Foley · hematuria / clot risk
- 12 Fr · delicate anatomy / pediatric
- Coude tip · BPH or prior difficult male insertion
- Straight-cath only · single-drainage indication
- Sterile fenestrated drape · sterile gloves
- Iodophor or chlorhexidine swabs (per policy)
- 2% lidocaine jelly (urethral anesthetic)
- Sterile water-based lubricant
- 10 mL pre-filled sterile water syringe
- Drainage bag with anti-reflux valve
- StatLock or securement strap (medial thigh)
- 01Position & light. Supine, knees flexed and abducted (frog-leg), sterile fenestrated drape, light source aimed to illuminate the meatus.
- 02Sterile field. Hand hygiene, sterile gloves, sterile drape. Open kit, pour iodophor or chlorhexidine, draw sterile water into pre-attached syringe (do not separate before testing balloon if institutional policy requires — many UCI kits ship pre-tested).
- 03Labial spread & meatal prep. Non-dominant hand spreads the labia (now contaminated, remains in position). Three swabs front-to-back, one stroke per swab, center swab last.
- 04Advance midline. With dominant sterile hand only, advance the lubricated catheter along the vertical midline. Urine returns at ~2–3 in. Advance another 1–2 in before balloon inflation.
- 05Vaginal misplacement. If the catheter passes without urine return and without resistance, suspect vaginal misplacement. Leave it as a landmark and use a fresh sterile catheter in the correct tract — never reuse the contaminated catheter.
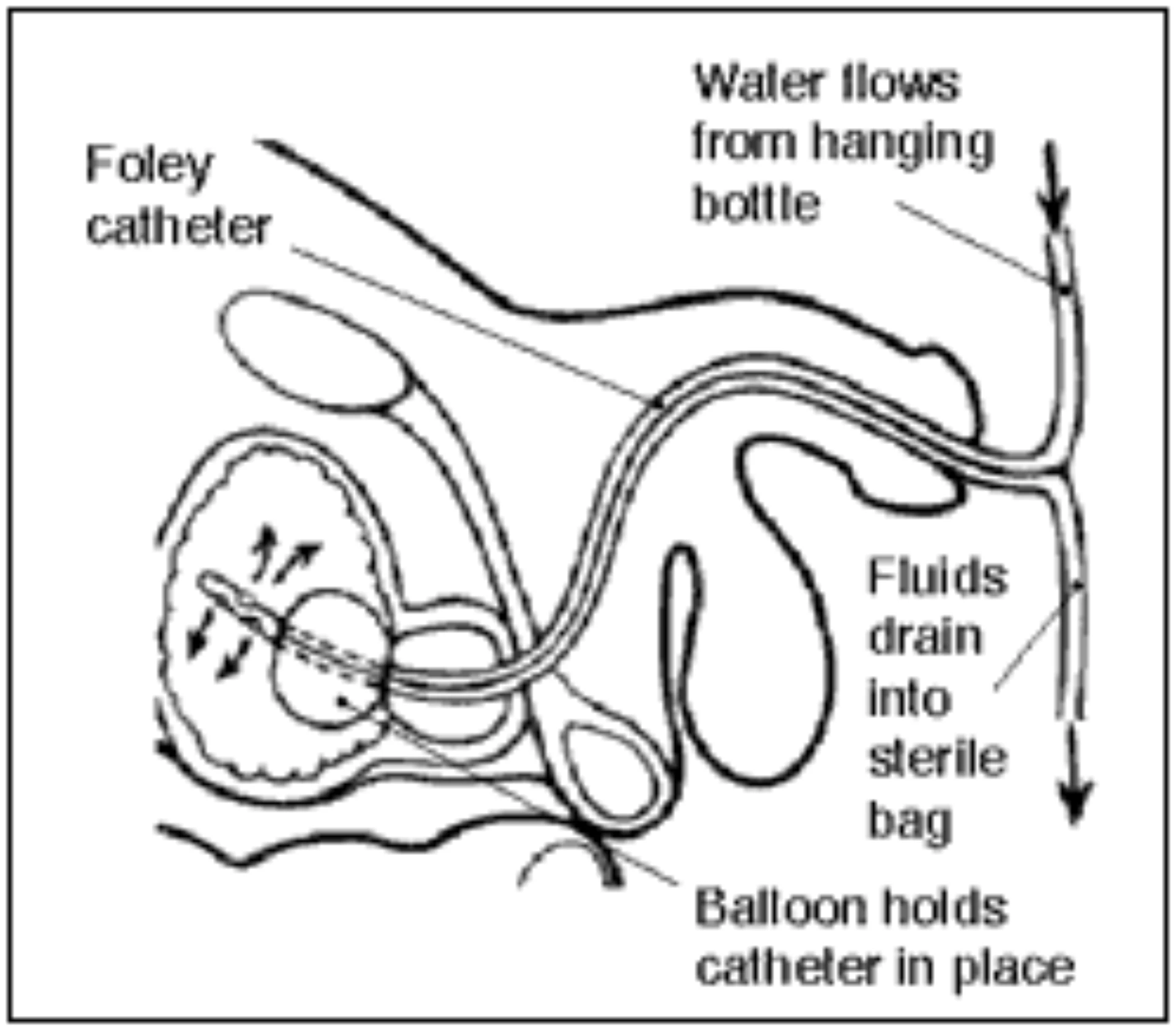
- 06Inflate & seat. Inflate with 5–10 mL sterile water. Gentle traction until balloon seats at bladder neck. Attach closed drainage system.
- 01Position & foreskin. Supine, legs extended, draped. In uncircumcised patients, retract the foreskin — and remember this for step 06. Grasp the shaft with the non-dominant hand (now contaminated) and lift the penis perpendicular (~90°) to straighten penile + bulbar urethra.
- 02Meatal prep. Three swabs in concentric circles, center-out. Meatus first, then surrounding glans.
- 03Lidocaine instillation. Instill 5–10 mL of 2% lidocaine jelly into the urethra. Dwell 5–10 minutes — meaningful difference at the prostatic curve. (Institutional norm per UCI Nursing Ed / Marino Ch 41.)
- 04Advance at 90°. Steady gentle pressure. The penile and bulbar segments accept the catheter easily. Never force against firm resistance.
- 05Drop to 45° at the prostate. When you feel the prostatic resistance, lower the penis to ~45° toward the feet. This aligns the catheter with the membranous and prostatic urethra. Urine returns at ~6–8 in. Advance another 1–2 in before balloon inflation.
- 06Inflate · seat · return foreskin. Inflate with 5–10 mL sterile water. Gentle traction. Return the foreskin to its anatomic position — failure to do so causes paraphimosis, a urologic emergency.
Confirm urine return
before you inflate.
Inflating in the urethra creates a false passage at minimum and a long-term stricture at worst. If you've advanced to the hub with no urine return, withdraw, re-prep, fresh catheter.
Firm resistance + BPH or stricture history = call urology. Adjunct steps first: lidocaine jelly 5–10 min dwell, Coude tip concave-up. Urology after one failed retry.
NEVER leave the foreskin retracted.
urethral injury we see in this institution.
- Secure to the medial thigh in all adults (current SHEA/IDSA practice — Patel 2022)
- StatLock or equivalent securement device · tape slides
- Drainage bag below the level of the bladder at all times · no dependent loops
- Closed drainage system — never disconnect for sampling
- Daily perineal care with soap and water · no antimicrobial agents needed
- No routine irrigation
- No routine prophylactic antibiotics
- No routine catheter exchange
- Yes — daily indication review with prompt removal
CAUTI.
Risk rises ~3–7% per day of dwell. NHSN-reportable. Bundle adherence + prompt removal are primary prevention.
Urethral injury.
Forced insertion against firm resistance is the dominant mechanism. Blood at meatus = stop. Urology consult.
False passage.
Premature balloon inflation in urethra or repeated forced attempts. Risks long-term stricture. Cystoscopic / IR retrieval.
Paraphimosis.
Unreturned foreskin in uncircumcised male = urologic emergency. Manual reduction or surgical release.
Bladder spasm.
Usually self-limited. Anticholinergics if severe. Re-check catheter not too small / over-inflated.
Meatal pressure ulcer.
From tight or kinked securement. Re-secure, off-load skin, daily perineal care.
Balloon rupture.
On removal — retained fragment. Cystoscopic retrieval. Document fragment count.
Catheter w/o indication.
A catheter placed without an accepted indication is the dominant driver of CAUTI. Indication discipline is the fix.
Forcing against firm resistance.
The dominant mechanism of urethral injury we see. Stop, lidocaine jelly dwell, Coude tip — and then urology after one failed retry. Never force.
Inflating before urine return.
A near-miss that becomes a stricture when missed twice. If catheter is at the hub with no return — withdraw, fresh catheter. Never inflate on hope.
Leaving the foreskin retracted.
Paraphimosis is a urologic emergency and is 100% preventable. The last step of male catheterization is always: return the foreskin.
No daily necessity review.
The pitfall that drives the institutional CAUTI rate. Ask every day: does this still need to be in? Pull the day the indication resolves.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of urinary catheter privilege | First 3 independent cases · per-case review within 30 d · aggregate at 3 · closed within 6 mo |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication or CAUTI event |
| Ad-hoc FPPE | Urethral injury · paraphimosis · CAUTI w/ bacteremia · non-indicated pattern | 3 subsequent cases reviewed; outcome a / b / c |
| Reinstatement | < 3 independent cases over 24 mo | Phantom skills checklist + 1 proctored live case (lapse is rare — high-volume procedure) |
- CAUTI rate < 1 / 1,000 catheter-days (UCI target)
- First-attempt success ≥ 80%
- Appropriate-indication rate 100%
- Daily-indication-review rate ≥ 95%
- Urethral injury / false passage rate — 100% per-case review on any occurrence
- Paraphimosis events — 100% per-case review, target zero
- Procedure-note completeness 100%
- 01Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections. CDC HICPAC. 2009 (reaffirmed 2017).
- 02Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated UTI in adults: 2009 IDSA international clinical practice guidelines. Clin Infect Dis. 2010;50(5):625–63. PMID 20175247.
- 03Patel PK, Advani SD, Kofman AD, et al. Strategies to prevent catheter-associated urinary tract infections in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. 2023;44(8):1209–1231. PMID 37620117.
- 04Septimus EJ, Arya LA, Crapanzano-Sigafoos R, et al. Prevention strategies for all hospital-onset urinary tract infections: best practice consensus recommendations. Open Forum Infect Dis. 2026;13(2):ofag060. PMID 41725706.
- 05Scruggs-Wodkowski E, Kidder I, Meddings J, Patel PK. Urinary catheter-associated infections. Infect Dis Clin North Am. 2024;38(4):713–729. PMID 39261137.
- 06Marino PL. Urinary catheters. In: The ICU Book, 4th ed. Lippincott Williams & Wilkins; Ch 41.
- 07Torbey MT, ed. Neurocritical Care, 2nd ed. Cambridge University Press; Ch 33 (bedside procedures).
- 08Bigelow Medical Service. Massachusetts General Hospital Handbook of Internal Medicine — Foley protocol. 2024–25 ed.
- 09The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 09aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 09bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 09cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 09dThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 10The Joint Commission. HR.01.06.01 (competence verified before care) · MS.08.01.01 / MS.08.01.03 (FPPE / OPPE). 2024.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.
- 12UCI Nursing Education. Aseptic technique & CAUTI-prevention modules. UCI Health; 2025.