NG/OG Tube
Insertion.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/11_*
- NG/OG tubes are among the most frequently misplaced bedside devices in adult inpatient care.
- Verification before first use is non-negotiable — chest X-ray is the gold standard before instillation of feeds, water, or medications (NPSA 2011 / AACN 2016).
- Air-bolus auscultation is no longer acceptable as a stand-alone verification — has produced fatal misfeeds.
- NG in suspected basilar skull fracture has caused intracranial placement and fatal CSF disruption — OG is mandatory here.
NPSA/2011/PSA002. Reducing the harm caused by misplaced nasogastric feeding tubes in adults.
Anatomy & route choice.
Describe upper aerodigestive anatomy; justify why insertion is straight back along the nasal floor — never angled toward the brow.
Indications & contraindications.
Differentiate accepted NCC indications; recognize basilar skull fracture as absolute contraindication to NG — select OG instead.
NEX measurement & insertion.
Measure NEX, position high-Fowler with chin tuck, lubricate, advance straight back, coordinate with swallow to pre-marked depth.
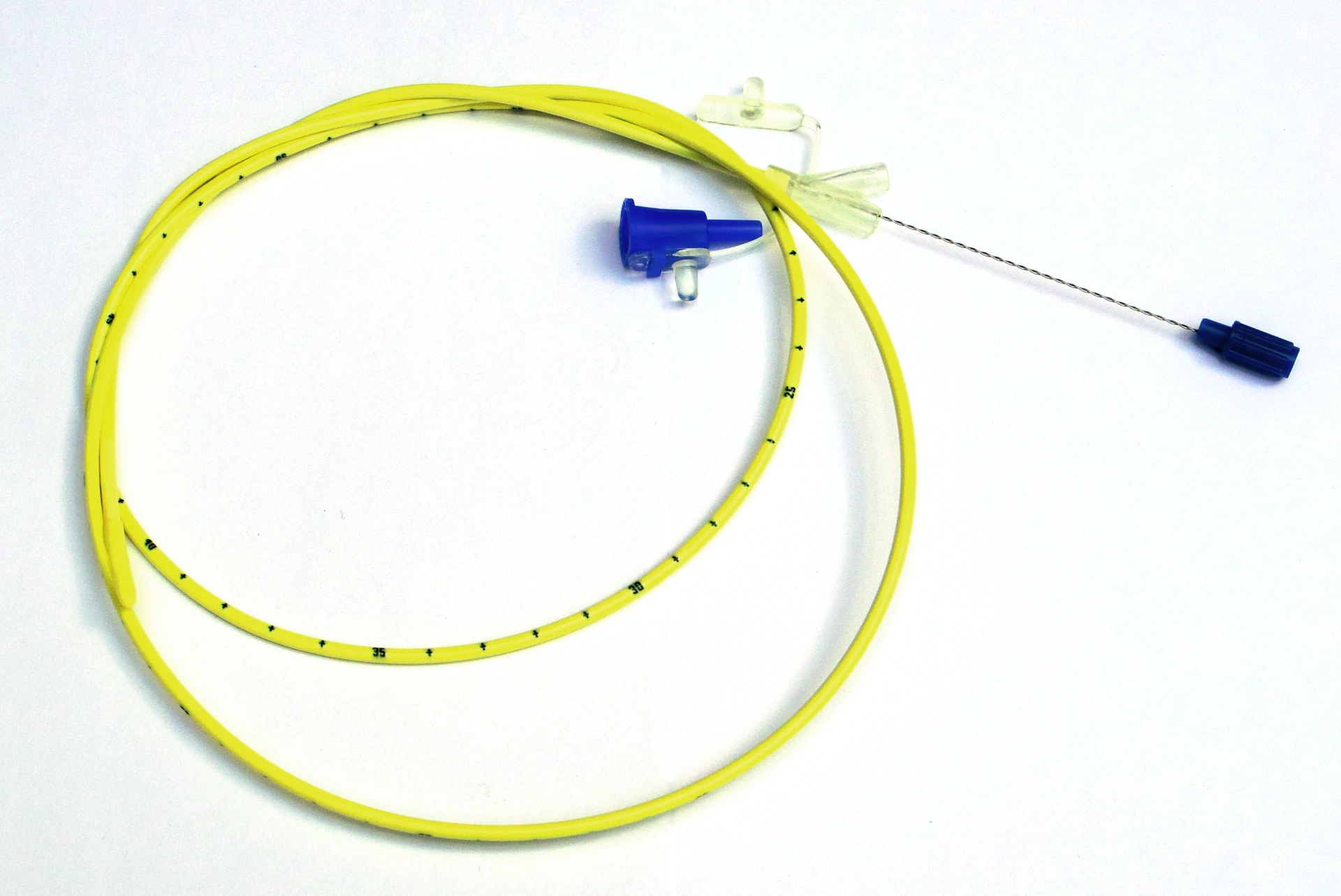
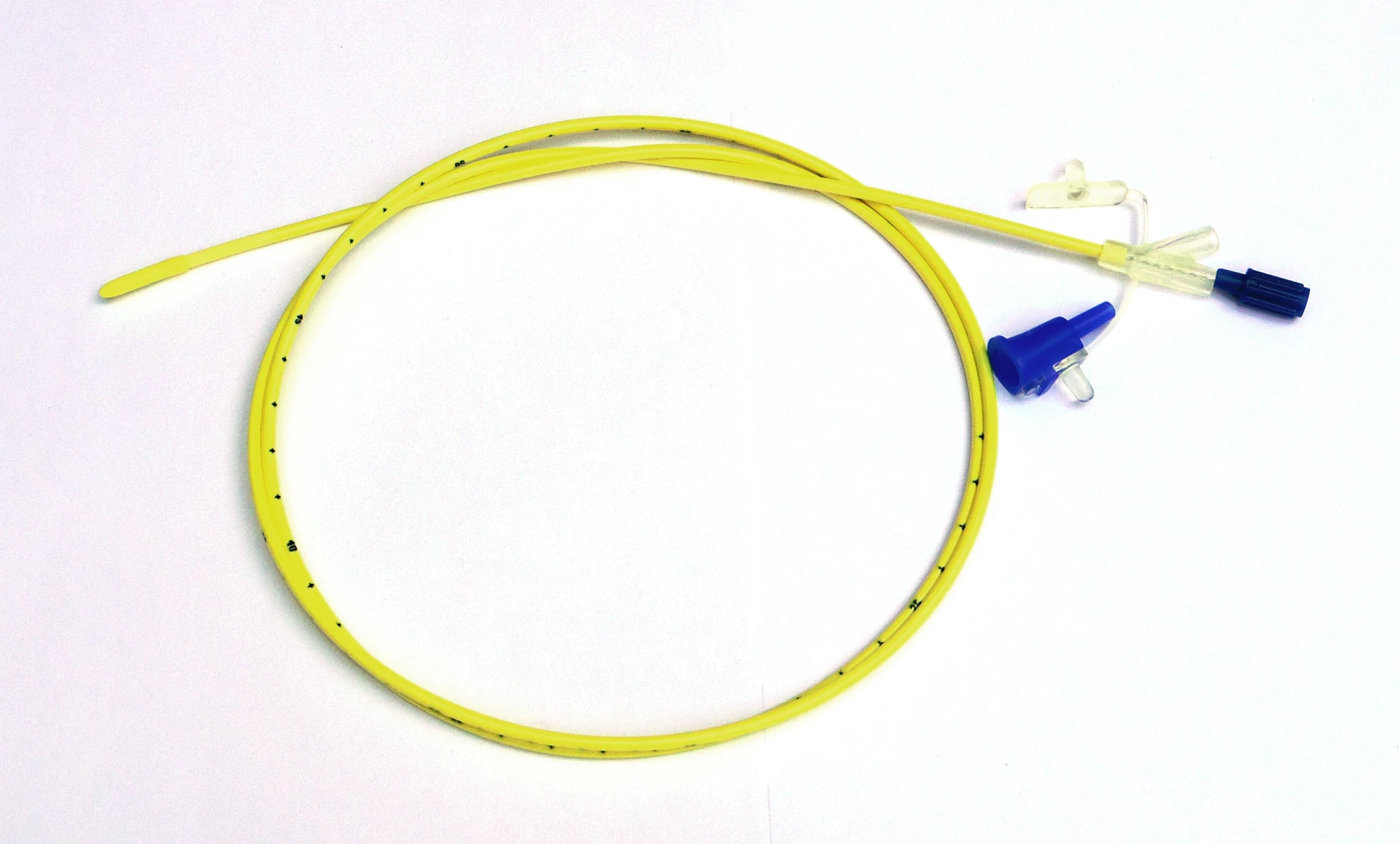
Tube selection.
Match tube and Fr size to indication — 14–18 Fr Salem Sump for decompression; 8–12 Fr small-bore weighted for feeding.
Radiographic confirmation.
Confirm gastric placement on KUB or chest X-ray before any feed or medication, per AACN 2016 — auscultation alone is insufficient.
Misplacement response.
Recognize cough / desaturation as tracheobronchial signals; withdraw immediately; hold feeds; escalate; disclose per UCI standards.
diaphragm.
spine.
the tip.
interpreting team.
- Gastric decompression — ileus, small-bowel obstruction, post-operative gastroparesis
- Gastric lavage — selected acute toxic ingestion or upper-GI bleed cases
- Enteric medication delivery in NPO patients unable to swallow safely
- Short-term enteral feeding when oral intake is contraindicated — intubated, GCS ≤ 8, status epilepticus on continuous infusion
Marino PL. The ICU Book, 4th ed. Ch 48. Wolters Kluwer; 2014.
- Post-operative SAH patient with ileus → decompression
- Intubated TBI patient · GCS 6 → enteral feeding initiation
- NPO status epilepticus patient on continuous AEDs → medication delivery
- Anything outside these buckets → escalate before placing
- Basilar skull fracture or suspected cribriform-plate injury — reported NG cases have caused intracranial placement, fatal
- Severe maxillofacial trauma with disrupted nasal architecture
NPSA/2011/PSA002. Reducing the harm caused by misplaced nasogastric feeding tubes in adults.
- Esophageal varices — coordinate with GI before insertion
- Recent upper-GI surgery — coordinate with surgical team
- Known stricture or esophageal pathology
- Coagulopathy or active anticoagulation — weigh epistaxis risk
- Chronic nasal obstruction — switch nostril or convert to OG
- OG preferred — intubated, comatose, or unable to protect airway
- OG required — basilar skull fracture or midface trauma; never NG here
- NG preferred — awake, cooperative patient; better tolerated for prolonged use
- Salem Sump 16–18 Fr — double-lumen decompression; blue pigtail vents to atmosphere · never clamp the blue pigtail
- Levin tube — single-lumen; short-term suction only; not preferred long-term (mucosal trauma)
- Small-bore weighted feeding tube 8–12 Fr with stylet — weighted tip aids transpyloric passage
- Too small for decompression → clogs · too large for feeding → alar-rim pressure injury
- Salem Sump (decompression) or Levin tube
- Small-bore weighted tube (feeding)
- Water-soluble lubricant · never oil-based
- 60-mL catheter-tip syringe
- Emesis basin · tape · pH strips
- Cup of water + straw if awake & not aspiration-risk
- Capnography / colorimetric CO2 if available
- Penlight for posterior pharynx inspection
- Suction setup at bedside · Yankauer + canister
- CXR access for post-placement confirmation
- 01Verify the patient. Two identifiers, allergies, indication. Re-screen for new basilar-skull-fracture findings or recent epistaxis.
- 02Informed consent. Procedure, expected discomfort (gagging, nasopharyngeal irritation, watering eyes), risks (epistaxis, malposition, aspiration, rare esophageal injury). Surrogate decision-maker if patient lacks capacity.
- 03Name the stop signal. For awake patients — raised hand, tap on rail. Rehearse it. Document that the patient understands they may abort.
- 04Universal Protocol time-out. Per TJC UP.01.03.01 — correct patient, correct procedure (NG vs OG), correct side (which nare), equipment ready, suction at bedside.
- 05Document indication and route in EHR. The chart entry starts the maintenance and verification clock.
- Hold all feeds and medications immediately
- Remove the tube if position cannot be verified radiographically
- Escalate to attending
- Disclose per UCI event-reporting standards
TJC Hospital Accreditation Standards · 2024.
- Head of bed 45–90° (high Fowler) — closes airway, opens esophagus
- Chin tucked to chest during advancement — directs tube posteriorly toward esophagus
- Suction setup and emesis basin within reach before advancing
- If intubated/sedated — head midline, verify cuff inflation before OG attempt
- Tip of nose → earlobe → xiphoid process
- Mark the tube at the measured length with tape or marker
- Adult NEX typically 50–60 cm — expect this depth at the nostril once seated
- Re-measure if anatomy makes standard NEX implausible
- CRITICAL ACTION · documented before insertion
- Apply water-soluble lubricant to the distal 4–6 inches of the tube
- Never mineral oil or petroleum-based lubricant — aspiration causes lipid pneumonitis
- Inspect tube for defects before insertion
- For feeding tubes with stylet — flush to confirm patency before insertion
- Stylet handling per institutional protocol — never re-insert a stylet once the tube is past the carina
Boullata JI et al. ASPEN safe practices. JPEN. 2017;41(1):15–103 · PMID 27815525
Step 03 — angle straight back
along the nasal floor.
- Direct the tube straight back along the nasal floor — parallel to the palate
- Resistance at 5–7 cm usually means turbinate contact — withdraw, redirect, try the contralateral nare
- Stop immediately on sudden give or any CSF-like drainage — withdraw and image
- Do not angle upward toward the brow — turbinates bleed
- Do not use the nasal route in suspected basilar skull fracture — intracranial NG placement is reported and fatal
Use OG.
NPSA/2011/PSA002 · OpenStax A&P 2e · Fig 22.4 · CC BY 4.0
Coordinate with
swallowing.
- At the oropharynx — pause and instruct
- If safe — small sips of water through a straw; advance during each swallow
- Each swallow closes the airway via epiglottic deflection and opens the UES
- If unsafe to swallow (NPO, dysphagia, intubated) — advance steadily with chin tucked
- Persistent cough / dyspnea / voice change / desaturation → STOP, WITHDRAW, REASSESS · never advance through respiratory distress
Past the tongue,
midline.
- Inspect oropharynx with penlight — tube passes midline, not coiled
- Tube curling in the mouth → withdraw to oropharynx and re-advance with swallow
- Continue advancing to the pre-marked NEX length
- For OG — advance past midline of tongue; jaw-lift or laryngoscope assist if intubated/sedated
- Tape to the nose without pressure on the alar rim — pressure injury is preventable
- Document length at the nostril (e.g., 55 cm at the nare) — this is the daily-rounding reference
- Record nare used, attempts, patient tolerance, external length in the procedure note
- Do not connect to suction or feeding until radiographic confirmation is in hand
- Secure to the cheek, never to the nose
- Document length at the incisor
- Indicated for basilar-skull / cribriform / severe maxillofacial trauma — never use NG route here
NPSA/2011/PSA002. Reducing the harm caused by misplaced NG feeding tubes in adults.
Confirm position on X-ray
before any feed.
Tip sits below the diaphragm, to the left of the spine, with the gastric bubble around the tip. Read with the interpreting team.
Air-bolus auscultation has produced fatal misfeeds and is not a stand-alone confirmation method.
placement confirmation is verified.
NPSA/2011/PSA002 · Boeykens K et al. Crit Care. 2023;27(1):317 · PMID 37596615
| Adjunct | What it tells you | What it does not tell you |
|---|---|---|
| Gastric pH | pH ≤ 5.5 supports gastric placement; pH > 6 raises concern for respiratory or small-bowel position. | PPI / H2 acid suppression blunts the discriminator. Not definitive. Repeat at first confirmation and before each subsequent feed (ASPEN 2017). |
| Capnography / colorimetric CO2 | Absence of CO2 helps rule out tracheal placement during insertion. | Presence of CO2 is a strong tracheal / bronchial signal — withdraw immediately. |
| Auscultation | DO NOT USE as a primary or sole verification method. | Cannot reliably distinguish gastric / esophageal / pulmonary placement — NPSA 2011 / AACN 2016 explicitly advise against. |
| EM placement (Cortrak) | Bedside trace can support placement during advancement. | Does not replace radiographic confirmation for feeding tubes per NPSA / AACN. |
AACN. Crit Care Nurse. 2016;36(2):e8–e13 · PMID 27037348 · Boullata JI et al. JPEN. 2017;41(1):15–103 · PMID 27815525
Tracheobronchial malposition.
Feed or medication into airway → chemical pneumonitis, aspiration pneumonia, death. CXR before any feed.
Intracranial placement.
NG in basilar skull fracture — reported and fatal. Use OG whenever skull-base injury is suspected.
Epistaxis.
Turbinate contact from upward angulation. Withdraw, redirect, contralateral nare. Pack if severe.
Esophageal perforation.
Rare. Forced advancement against resistance. Stop on unexpected resistance — escalate.
Sinusitis.
Prolonged NG dwell. Consider OG conversion if > 7–10 days and clinical signs develop.
Alar-rim pressure ulcer.
Tape tension on the nasal alar rim. Daily skin check; rotate tape position; use foam securement.
Daily — measure external length each shift.
Re-image with CXR if dislodgement is suspected. pH at each feed as adjunct.
Daily — is the tube still indicated?
Flush 30 mL water before/after meds and q4–6h on continuous feeds. Remove as soon as not needed.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of NG/OG privilege | First 3 independently performed cases · per-case review within 14 days · aggregate at 3 · closure within 6 months |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review on any misplacement flag |
| Trigger review | Misplacement · feed before CXR · absent skull-base screen in trauma patient | Ad-hoc focused review · minimum 3 subsequent cases |
| Reinstatement | < 5 independent cases over rolling 24 mo | Stream B skills checklist + 1 proctored live case rated Independent |
- Misplacement rate zero-tolerance
- X-ray confirmation before any feed/med 100%
- Basilar-skull screen documented (head/face trauma) 100%
- Documentation completeness — route, Fr, NEX, length, CXR ref, pH, complication 100%
- Complication rate — per-case review on any occurrence
- 01AACN. Initial and ongoing verification of feeding tube placement in adults. Practice Alert. Crit Care Nurse. 2016;36(2):e8–e13. PMID 27037348.
- 02NPSA. Reducing the harm caused by misplaced nasogastric feeding tubes in adults. NPSA/2011/PSA002. National Patient Safety Agency; March 2011.
- 03Wolter G, Naqvi ZU, Jalali A, et al. Intracranial injury following nasogastric tube placement after skull base surgery: a case report and systematic review. Cureus. 2025;17(7):e89085. PMID 40896069.
- 04Elmahdi A, Eisa M, Omer E. Aspiration pneumonia in enteral feeding: a review on risks and prevention. Nutr Clin Pract. 2023;38(6):1247–1252. PMID 37227191.
- 05Boeykens K, Holvoet T, Duysburgh I. Nasogastric tube insertion length measurement and tip verification in adults: a narrative review. Crit Care. 2023;27(1):317. PMID 37596615.
- 06Boullata JI, Carrera AL, Harvey L, et al. ASPEN safe practices for enteral nutrition therapy. JPEN J Parenter Enteral Nutr. 2017;41(1):15–103. PMID 27815525.
- 06aCompher C, Bingham AL, McCall M, et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: the American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2022;46(1):12–41. PMID 34784064.
- 06bPerry A, Kaiser J, Kruger K, et al. ENA clinical practice guideline synopsis: gastric tube placement verification. J Emerg Nurs. 2024;50(2):301–304. PMID 38453344.
- 07Marino PL. Marino's The ICU Book, 4th ed. Ch 48 (enteral access). Wolters Kluwer; 2014.
- 08MGH Internal Medicine Housestaff Manual, 2024-25 ed. Nasogastric section. MGH Dept of Medicine.
- 09The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 09aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 09bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 09cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 09dThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 10The Joint Commission. HR.01.06.01 — competence verified before care. TJC Hospital Accreditation Standards; 2024.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.
- 12OpenStax College. Anatomy & Physiology 2e. Figures 22.4 (nasal anatomy) & 23.13 (GI). CC BY 4.0.
≥ 10/12
all 4 critical † · Independent
per Training Plan
→ Credentials → MEC → Board