Peripheral IV
Placement.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
- Most-performed invasive procedure in the hospital — aggregate harm signal is real.
- Failed attempts delay fluids, antibiotics, contrast, and clot lysis — measurable.
- Vesicant-through-PIV (norepinephrine, CaCl2, hypertonic saline) drives the catastrophic-extravasation tail.
- INS 2024 sets the practice floor for catheter selection, dwell time, and dressing care.
Nickel B. Crit Care Nurse. 2019;39(1):61–71 · PMID 30710037
Indications & vesicant exclusion.
Differentiate PIV-appropriate from central-only infusates — vasopressors, concentrated electrolytes, TPN, pH <5 or >9, osmolarity >900 mOsm/L.
Gauge & site selection.
Match gauge to indication per INS 2024 (14–24 g) and apply the distal-to-proximal forearm-preferred site hierarchy.
Landmark insertion.
Anchor, bevel-up at 10–30°, flash, drop to 5–10°, advance off stylet, release tourniquet, flush, secure.
Ultrasound-guided rescue.
Apply the Dawson rule (≥50% intravascular) and INS pre-scan thresholds for difficult-access PIV.
Complication recognition.
Differentiate infiltration from extravasation; recognize phlebitis, hematoma, arterial puncture, nerve injury early.
Documentation & escalation.
Document site, gauge, attempts, US use, flush, dressing; escalate vesicant orders to central / midline access.
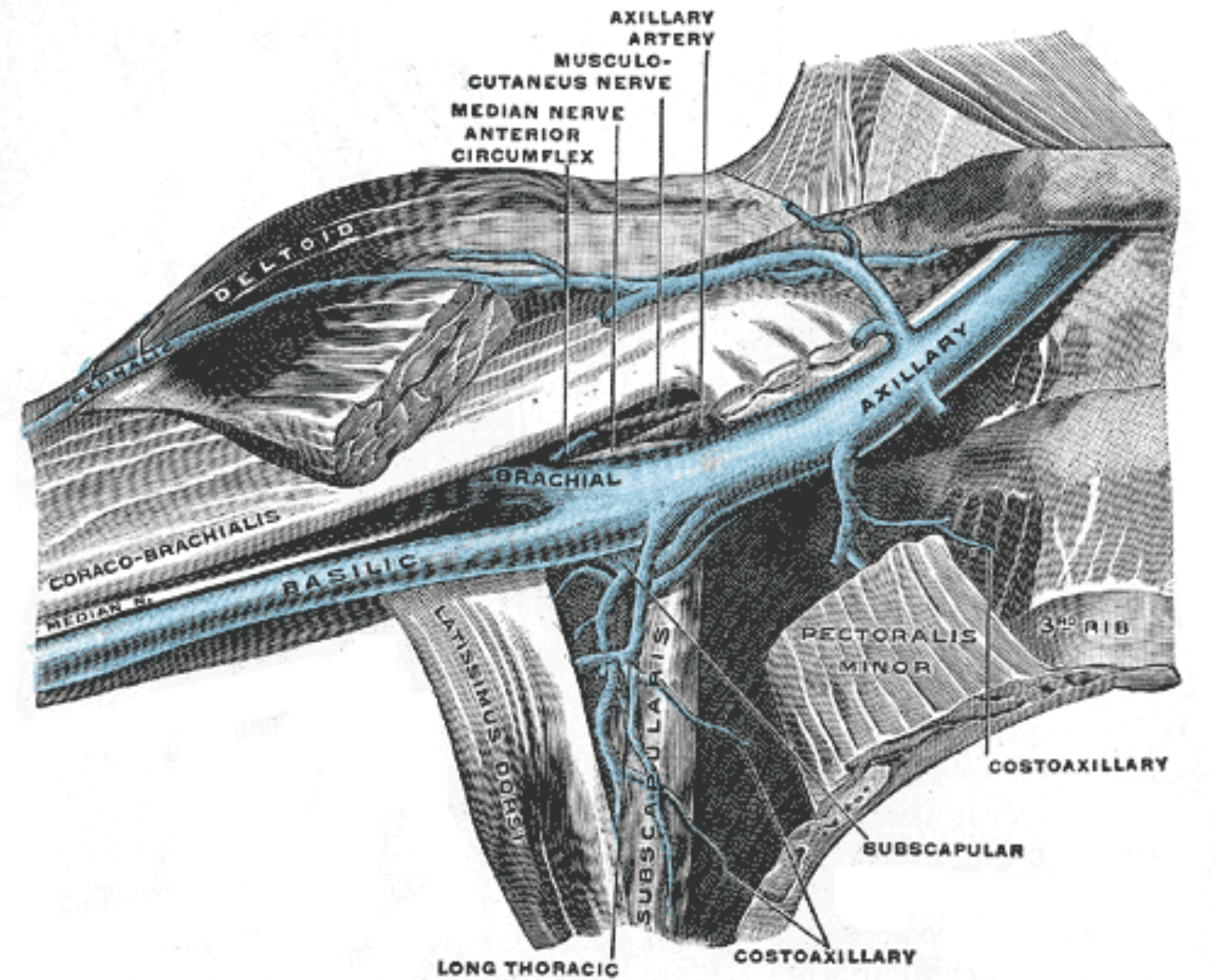
- Cephalic (radial side) · basilic (ulnar side) · median antebrachial (between) — long, straight segments, away from flexion.
- Distal to proximal — start where you can live with failure, escalate up the arm only when needed.
- Avoid the AC fossa for routine access — flexion kinks the catheter, blunts flow, shortens dwell.
- Hand veins acceptable when forearm fails — higher pain, lower dwell, more infiltration; avoid near radial artery / median nerve at the wrist.
- Skip the affected limb — mastectomy-ipsilateral, AVF extremity, paretic limb, lymphedema side, burned or infected skin.
- No lower-extremity PIV in adults — DVT risk and dwell are both worse.
| Gauge | Color | Indication | Site preference |
|---|---|---|---|
| 14 g | Orange | Major trauma · massive transfusion · flow rates ~270 mL/min | AC fossa or large forearm vein |
| 16 g | Grey | Trauma · rapid transfusion · flow rates ~180 mL/min | AC fossa or large forearm vein |
| 18 g | Green | Power-injection contrast · blood products · rapid resuscitation | AC fossa or large forearm — default trauma-bay gauge |
| 20 g | Pink | Most adult inpatients — maintenance fluids, antibiotics, routine meds | Forearm cephalic / basilic / median |
| 22 g | Blue | Small veins · elderly · oncology with prior chemotherapy | Forearm or dorsal hand — smallest gauge meeting the indication |
| 24 g | Yellow | Extremely small veins · fragile skin · pediatric | Dorsal hand · short dwell expected |
- Short-term IV fluid, electrolyte, and crystalloid resuscitation
- Non-vesicant medications — antibiotics, antiemetics, analgesics (verify each agent)
- Iodinated contrast for CT (pump-rated catheters, typically 18–20 g in AC fossa)
- Bridge access while midline / PICC / CVC is being arranged
- Access-deficient patient with no central indication
- Vasopressors — norepinephrine, epinephrine, vasopressin, phenylephrine (extravasation → necrosis)
- Concentrated electrolytes — KCl > 10 mEq/100 mL · hypertonic saline ≥ 3% prolonged · CaCl2
- Chemotherapy vesicants — anthracyclines, vinca alkaloids, mitomycin (oncology central only)
- TPN (PPN acceptable short-term peripherally)
- pH < 5 or > 9 · osmolarity > 900 mOsm/L — central / midline only
- 01Verbal consent. Indication, expected sensation ("sharp scratch, then pressure"), what to report during (burning, paresthesias) and after (swelling, redness, leaking, pain).
- 02Allergy & access history. Chlorhexidine, latex, adhesives, prior contrast reactions · recent draws, blown veins, indwelling lines, AVF laterality, mastectomy side.
- 03Site choice confirmed. Avoid mastectomy-ipsilateral arm, AVF extremity, paretic limb, lymphedema side, infected or burned skin.
- 04Infusate appropriateness. Confirm ordered agents are PIV-appropriate — flag vesicants, vasopressors, CaCl2, hypertonic saline, IV contrast. Escalate before puncture.
- 05Time-out called. Per TJC UP.01.03.01 — right patient, right indication, right extremity, allergies reviewed, consent confirmed.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
probe.
catheter.
rule.
thresholds.
- Catheter-over-needle, 14–24 g (BD Insyte Autoguard or equivalent)
- Tourniquet
- Chlorhexidine 2% / alcohol 70% applicator
- Saline-primed extension set (T-connector or saline lock)
- 10 mL preservative-free 0.9% saline flush
- Transparent semipermeable dressing (CHG-impregnated for high-risk sites)
- Tape · dressing label (date / time / gauge / initials)
- Non-sterile gloves
- Sharps container at bedside
- Warm compress for difficult access
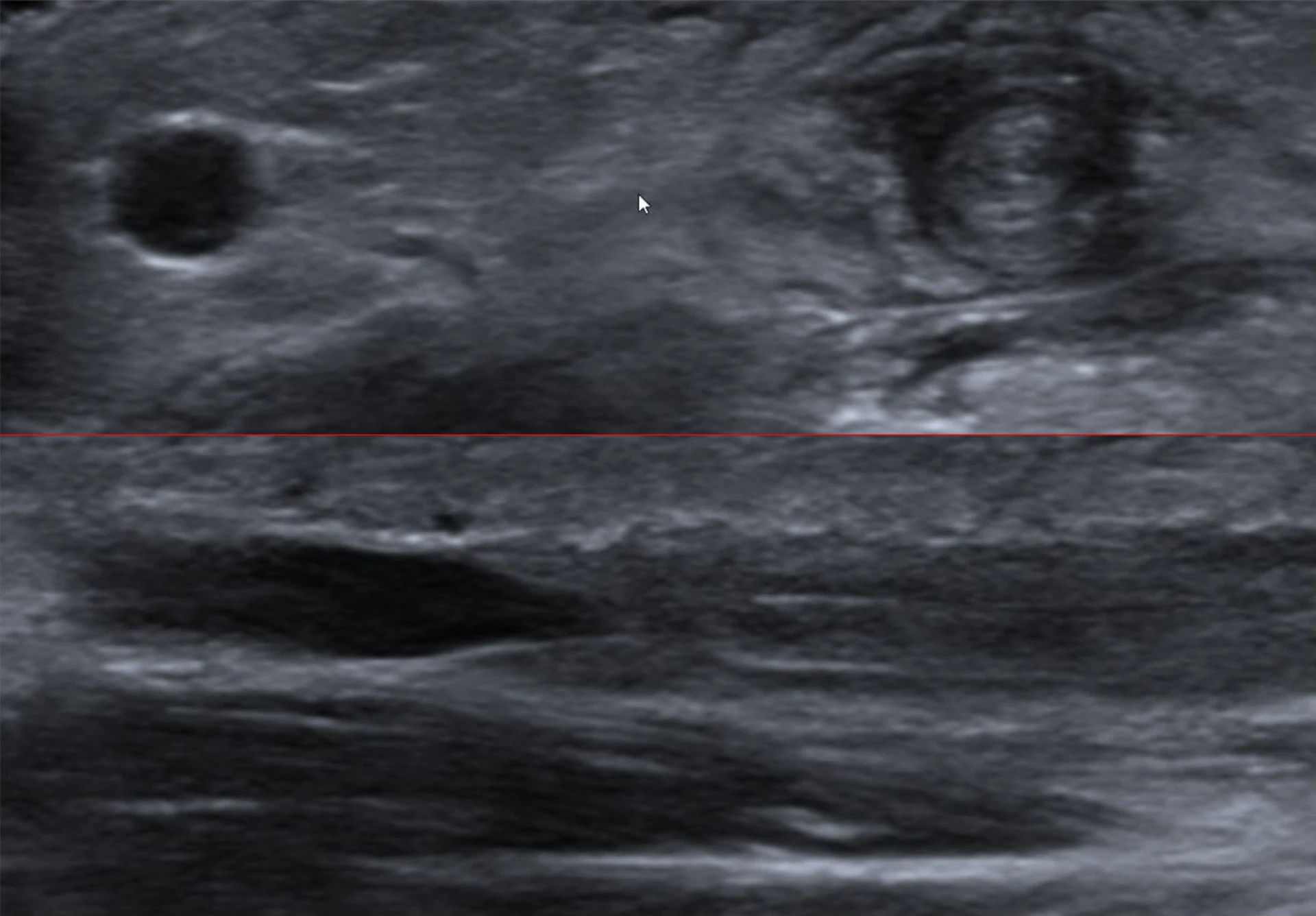
- High-frequency linear probe (10–15 MHz)
- Sterile probe sleeve · sterile gel
- Long catheter — ≥ 4.5 cm, often 6–8 cm for upper arm targets
- Basilic / brachial / cephalic in the proximal upper arm are the typical US targets
- Short-axis approach with dynamic tip tracking
- Apply tourniquet 4–6 in proximal to planned puncture — tight enough to engorge, loose enough to leave a radial pulse.
- Palpate for a soft, bouncy, straight segment — caliber and patency matter more than surface visibility.
- Chlorhexidine 2% / alcohol 70% — concentric circles, center out, 30 s scrub + 30 s air-dry. No blotting, no fanning.
- Tourniquet stays on ≤ 2 min total — beyond that → hemoconcentration, false lab values.
- If you re-palpate the prepped skin with non-sterile gloves — re-prep.
Anchor ·
bevel up.
- Non-dominant thumb 2–3 cm distal to puncture — traction along long axis, prevents rolling
- Bevel up · catheter tip aligned to long axis of vein
- Approach angle 10–30° on standard adult forearm
- Warn before contact — "sharp scratch coming"
Flash ·
drop · advance.
- Advance until give + flashback in chamber — stylet in lumen, catheter not yet
- Drop angle to 5–10°, advance unit 1–2 mm further
- Hold stylet steady; advance catheter off stylet with dominant hand
- If flash stops or pulses — vein transfixed; withdraw, reassess
Seat to
the hub.
- Lower angle flush with skin · advance catheter to hub in single smooth motion
- Mild resistance at valves expected — never force; rotate / small flush to open
- Partial seating = most common cause of early infiltration
- Do not flush before tourniquet release

- Non-dominant thumb anchoring skin distal to the planned puncture — traction along vein long axis
- Catheter held in dominant hand · bevel oriented up
- Approach angle on a typical adult forearm — flatter for superficial, steeper for deep
- Stylet still partially seated · operator's eyes on the flash chamber, not the skin
- Free hand stays ready to retract the stylet, advance the catheter, and engage safety
- Release the tourniquet first. Then engage the safety stylet retraction mechanism — sharps protection before anything else.
- Connect a saline-primed extension set
- Flush 3–5 mL of preservative-free 0.9% saline slowly
- Observe for resistance, swelling, pain at the site — if any, pull the catheter
- Confirm: no wheal, no surrounding induration, smooth flush
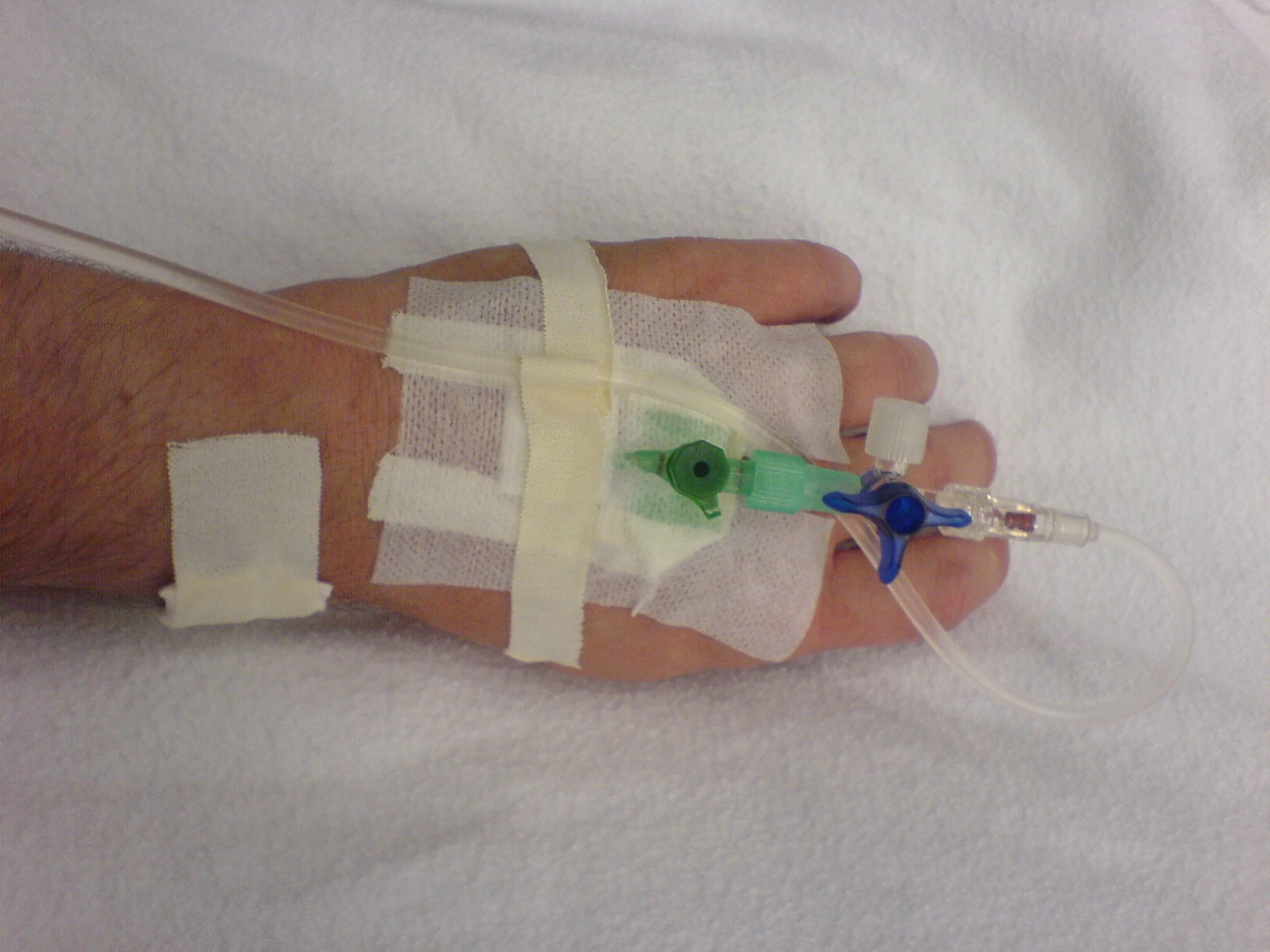
- Loop the extension set away from puncture — strain relief
- Transparent occlusive dressing over insertion site
- Label dressing: date · time · gauge · initials
- Document in EMR: site, laterality, gauge, attempts, US use, flush, dressing, baseline skin/extremity exam

- Indication — after two failed landmark attempts, or no peripheral vein palpable
- Probe — high-frequency linear, 10–15 MHz
- Target — basilic and brachial veins in proximal upper arm (typical); cephalic above AC also
- Catheter — long, ≥ 4.5 cm, often 6–8 cm
- Approach — short-axis · dynamic tip tracking · "bee-sting" view
- Thread under direct visualization — advance catheter beyond bevel into lumen
≥ 50% of catheter intravascular for adequate dwell · vein depth < 1.5 cm · diameter > 3 mm · catheter length 1.75–2.5 in.
Infiltration vs extravasation
— different response.
Non-vesicant fluid in subcutaneous tissue. Site is cool, soft, swollen; patient reports tightness. Stop infusion. Remove catheter. Elevate. Warm or cool compress per agent. Document.
Vesicant in tissue. Site is dusky, blistered, painful. Stop infusion. Leave catheter in. Aspirate residual drug from hub. Antidote per agent. Photograph. Notify pharmacy + primary team.
you pull the catheter.
INS. J Infus Nurs. 2024;47(1S):S1–S285
Infiltration.
Non-vesicant in tissue · cool, soft swelling. Stop, remove, elevate, compress per agent.
Extravasation.
Vesicant in tissue · dusky, blistered. Stop, leave catheter, aspirate, antidote, photograph.
Phlebitis.
Pain, erythema, palpable cord. Mechanical / chemical / infective. Remove, elevate, warm; replace elsewhere.
Hematoma.
Local bruising at puncture or post-removal. Pressure + elevation; rarely requires intervention.
Arterial puncture.
Bright pulsatile blood. Withdraw, hold pressure, reassess; rarely requires vascular consult.
Nerve injury.
Sudden electric paresthesia on puncture (median at wrist, radial at thumb). Withdraw immediately, document, neuro check.
Catheter-related BSI.
Uncommon with short PIV; rises sharply after 96 h dwell with poor dressing care. Remove on signs of infection.
Air embolism.
Prevented by priming the extension set and capping ports. Trendelenburg + left lateral decubitus if suspected.
Vesicant through a PIV.
Norepinephrine, CaCl2, hypertonic saline, chemo vesicants — these belong central / midline. Escalate the order before you puncture; do not run and document later.
Flushing into a tourniqueted limb.
Release the tourniquet before you flush. Flushing into closed venous outflow drives infusate into soft tissue — a wheal at the site is the tell.
Missed mastectomy / AVF history.
Skipping the time-out because PIV "feels low-stakes" is how the wrong arm gets cannulated. The history check is the discipline.
Three blind sticks before escalation.
After two failed landmark attempts — ultrasound, midline, or central. Not a third blind puncture, not a colleague's hands on the same arm.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of PIV privilege | First 5 independent placements · aggregate review by APP Director + CRNI · closed within 3 mo |
| OPPE | Continuous baseline · TJC MS.08.01.03 | Every 6 mo · 10% sample (min 2, max 10) · 100% review on any extravasation event |
| Trigger | Vesicant extravasation · contrast-extravasation w/ compartment · 2+ failures w/ harm in 90 d · safety event | Ad-hoc focused review per §3 structure · min 5 subsequent cases |
| Lapse | < 10 PIVs over 24 mo | Repeat skills checklist + 1 proctored case rated Independent |
- First-attempt success rate ≥ 75%
- Extravasation rate near zero · 100% per-case review on any
- Documentation completeness 100% (site, gauge, attempts, US use, flush, dressing, baseline exam)
- Appropriate-medication-for-access rate 100% · institutional exception tracked separately
- Time-out per TJC UP.01.03.01 documented 100%
- 01Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2024;47(1S Suppl 1):S1–S285.
- 02Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2021;44(1S):S1–S224. PMID 33394637.
- 03Egan G, Healy D, O'Neill H, et al. Ultrasound guidance for difficult peripheral venous access: systematic review and meta-analysis. Emerg Med J. 2013;30(7):521–6. PMID 22886890.
- 04Nickel B. Peripheral intravenous access — applying infusion therapy standards of practice to improve patient safety. Crit Care Nurse. 2019;39(1):61–71. PMID 30710037.
- 04bBahl A, Alsbrooks K, Zazyczny KA, et al. An improved definition and SAFE rule for predicting difficult intravascular access (DIVA) in hospitalized adults. J Infus Nurs. 2024;47(2):96–107. PMID 38377305.
- 04cStefanos SS, Kiser TH, MacLaren R. Management of noncytotoxic extravasation injuries: a focused update on medications, treatment strategies, and peripheral administration of vasopressors and hypertonic saline. Pharmacotherapy. 2023;43(4):321–337. PMID 36938775.
- 05Marino PL. Marino's The ICU Book, 4th ed. Wolters Kluwer; 2014. Ch 1 & 3 — vascular access & vesicant pharmacology.
- 06Lee K, ed. The NeuroICU Book, 2nd ed. McGraw-Hill; 2018. Ch 34 — neuro-ICU procedures.
- 07Massachusetts General Hospital. Internal Medicine Housestaff Manual, 2024–2025 ed. Section: US-guided peripheral IV.
- 08Massachusetts General Hospital. Department of Medicine Point-of-Care Ultrasound Manual ("Gray Book"), 2021–2022 ed.
- 09The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 09aThe Joint Commission. Universal Protocol UP.01.01.01 — preprocedure verification; use a standardized list (H&P, signed consent, nursing & preanesthesia assessment, labeled imaging, required equipment/devices). National Patient Safety Goals (HAP); effective January 2025.
- 09bThe Joint Commission. NPSG.01.01.01 EP 1 — use at least two patient identifiers (room number is not an identifier) before any treatment or procedure. National Patient Safety Goals (HAP); effective January 2025.
- 09cThe Joint Commission. NPSG.07.01.01 EP 1 — implement CDC and/or WHO hand-hygiene categories IA, IB, IC. National Patient Safety Goals (HAP); effective January 2025.
- 09dThe Joint Commission. NPSG.03.04.01 — label all medications, medication containers, and solutions on and off the sterile field (name, strength, amount, diluent, expiration). EP 4 requires two-individual verification when preparer ≠ administrator. National Patient Safety Goals (HAP); effective January 2025.
- 10The Joint Commission. HR.01.06.01 — staff are competent to perform their responsibilities. 2024.
- 11The Joint Commission. MS.08.01.01 / MS.08.01.03 — FPPE / OPPE requirements. 2024.
- 12California Code of Regulations. 16 CCR §1474 (CA BRN scope) · 16 CCR §1399.541 (CA PA scope).
- 13UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.