Punch
Biopsy.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/13_Punch_Biopsy/
One tool —
five diagnostic worlds.

- Standard 3–4 mm punch yields full-thickness epidermis, dermis, subcutis.
- Serious complications are technique-driven and preventable.
- AANEM 2026 places IENF density at Level A evidence for SFN diagnosis.
Indication selection.
Name the four canonical indications and the neurology-specific roles (SFN IENF density, cutaneous α-synuclein); recognize melanoma as a non-punch lesion.
Contraindications.
Screen for coagulopathy, thrombocytopenia < 50,000, active site infection, anatomic exclusion zones (face / hands / feet) and suspected melanoma.
Anesthetic technique.
Raise an intradermal lidocaine wheal; wait the canonical 1½–2 min for maximum anesthesia before advancing the punch.
Punch advance & lift.
Advance perpendicular to skin tension lines until the resistance change; lift with subcutaneous fat — never crush the dermal core.
Specimen handling.
Match fixative to indication — formalin / Michel / Zamboni / α-synuclein-specific medium — at the bedside, before the punch leaves the room.
Path follow-up loop.
Close the pathology loop on every specimen; document; escalate per UCI umbrella SP triggers when indicated.
~0.1 mm
Where melanocytes live.
- Stratum corneum down to basal layer
- Melanoma sits here — NOT a punch lesion (AAD: excisional)
- IENF terminals cross the epidermal–dermal junction
papillary + reticular · ~1–3 mm
Substrate for most diagnoses.
- Capillary loops · adnexal structures
- Inflammatory + vasculitic pathology lives here
- Small-fiber nerves · α-synuclein deposits
fat — required for full-thickness read
Clear the dermo-fat junction.
- Panniculitis & deep vasculitis need fat
- Punch must reach this layer or specimen is non-diagnostic
- SFN: distal-leg site, 10 cm above lateral malleolus
- Inflammatory dermatoses requiring tissue diagnosis — vasculitis, lichenoid reactions, drug eruptions, bullous disease
- Suspected non-melanoma skin cancers — basal cell, squamous cell, keratoacanthoma
- Dysplastic or complex nevi (per UCI canonical post-test, Q1)
- Persistent or evolving lesion that has failed empiric therapy — full-thickness architectural read
- Small-fiber neuropathy — IENF density on a distal-leg punch (10 cm proximal to the lateral malleolus); Level A evidence per AANEM 2026
- Cutaneous α-synuclein — multi-site protocol (posterior cervical / distal thigh / distal leg) for Parkinson disease, MSA, RBD work-up
- Suspected paraneoplastic vasculitis, dermatomyositis-spectrum eruptions, GVHD evaluation
Doppler K et al. Cutaneous neuropathy in Parkinson's disease. Acta Neuropathol. 2014;128(1):99–109 · PMID 24788821
- Suspected melanoma — refer for excisional with margins per AAD / NCCN
- Active local infection — defer until treated; biopsy through cellulitis distorts pathology & worsens infection
- Canonical UCI exclusion zones — face, hands, feet — refer to dermatology
- Uncorrected coagulopathy outside ASRA-PM acceptable range
- Anticoagulation — continue ASA in most; selective hold for warfarin / DOAC per ASRA-PM coordination with prescribing provider
- Thrombocytopenia — UCI institutional threshold ≥ 75,000 on Competence Assessment item 4; canonical post-test names < 50,000 as the contraindication line
- Cosmetically sensitive sites in non-consenting patients (permanent 3–4 mm scar)
- Immunocompromised patient with active site changes — coordinate with primary team
- Keloid history / Fitzpatrick IV–VI — counsel pre-procedure on dyschromia & scarring risk
- 01Consent documented. Indication, alternatives, scarring (every punch leaves a permanent 3–4 mm mark), dyschromia (Fitzpatrick IV–VI), bleeding, infection < 1%, non-diagnostic specimen possibility, repeat-biopsy contingency.
- 02Photograph & mark. Patient-consented clinical photo with scale marker. Mark the planned punch center with a surgical pen before prep and anesthetic — lidocaine + epi blanching obscures landmarks.
- 03Labs reviewed. PLT verification per Competence Assessment item 4: ≥ 75,000 or pre-procedure transfusion or MD clearance. INR if on anticoagulation; ASRA-PM 5th ed for hold-and-bridge planning.
- 04Hypersensitivity history. True lidocaine allergy is rare but real; document. Epinephrine avoided at fingers, toes, ears, nose tip, penis.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, site / side, equipment, consent confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
10 cm above lateral malleolus
full-thickness
NOT formalin
< 24 h ideal
- Disposable punch — 3 mm (SFN / cosmetic)
- Disposable punch — 4 mm (definitive dermpath)
- Disposable punch — 6–8 mm (panniculitis)
- 1% lidocaine ± epinephrine
- 25–27 g needle · 3 mL syringe
- Chlorhexidine 2% / alcohol 70%
- Sterile drape · non-sterile gloves OK for routine
- Adson forceps (without teeth)
- Iris scissors (curved)
- 4-0 or 5-0 nylon suture · needle driver
- Gauze · aluminum chloride 20%
- Electrocautery (if available)
- Petrolatum + non-stick pad + tape
- Surgical pen · scale marker for photo
Ajay Kumar Chaurasiya via Wikimedia · CC BY-SA 4.0
- Formalin 10% NBF — routine histopath, neoplastic, most inflammatory
- Michel medium — DIF (vasculitis, pemphigus, pemphigoid, DH, CTD)
- Zamboni / 2% PFA — SFN IENF density (AANEM 2026)
- Protocol-specific — cutaneous α-synuclein (Syn-One / equivalent)
Mark ·
lidocaine wheal.
- Mark site with surgical pen before anesthetic — wheal distorts anatomy
- 1% lidocaine ± epi · intradermal wheal ~1 cm
- Aspirate before injection; inject slowly
- Wait 1½–2 min per UCI Competence Assessment item 7 (up to 5 min for full epi vasoconstriction)
- Avoid epi at digits, ear, nose tip, penis
Punch ·
advance to resistance change.
- Stretch skin perpendicular to relaxed skin tension lines → oval defect, cleaner closure
- Punch perpendicular to surface; rotate one direction with steady downward pressure
- Advance until resistance lessens — punch has entered subcutaneous fat. Withdraw.
- Do not bottom out on bone / fascia
Zpuckr200 via Wikimedia · CC BY-SA 4.0
Match the fixative
to the indication.
10% neutral-buffered formalin — inflammatory dermatosis, neoplastic, drug eruption, most general derm.
Michel medium — vasculitis, pemphigus, pemphigoid, DH, CTD. Formalin destroys the immunoreactants.
Zamboni or 2% PFA — per AANEM 2026 SFN Task Force. Not formalin. Transport to neuropath lab < 24 h.
Protocol-specific medium — coordinate with neuropath / Syn-One before the punch. Posterior cervical / distal thigh / distal leg multi-site protocol.
= repeat biopsy.
Katzberg HD et al. Muscle Nerve. 2026;73(6):952–960 · PMID 41670166
Lift · cut ·
do not crush.
- Lift with Adson forceps grasping subcutaneous fat only — never dermis or epidermis
- If core does not pop up: hypodermic needle or fine-tooth forceps on fat (per Competence Assessment item 13)
- Cut base with curved iris scissors at the fat plane
- Crush artifact ruins the path read → non-diagnostic specimen
- Include subcutaneous fat in the specimen — full-thickness or non-diagnostic
- Place immediately into the indication-matched fixative; label at bedside with two identifiers
Hemostasis ·
closure · dressing.
- Direct gauze pressure × 60 sec — first-line hemostasis
- Aluminum chloride 20% for oozing; electrocautery if available
- Closure: 4 mm punches → single 4-0 or 5-0 nylon interrupted; 3 mm often heals by second intention
- Dressing: petrolatum + non-stick pad + tape · keep dry 24 h, then daily soap-and-water
- Suture removal: face 5–7 d · trunk 10–14 d · extremity 10–14 d
- Pre-schedule removal before patient leaves the room
- Site (anatomic location and laterality)
- Lesion description, duration, distribution
- Suspected differential — drives stain selection
- Prior treatments — topical / systemic steroids, biologics, immunosuppression
- Immunocompromise / pregnancy status where relevant
Incomplete requisitions drive non-diagnostic reads.
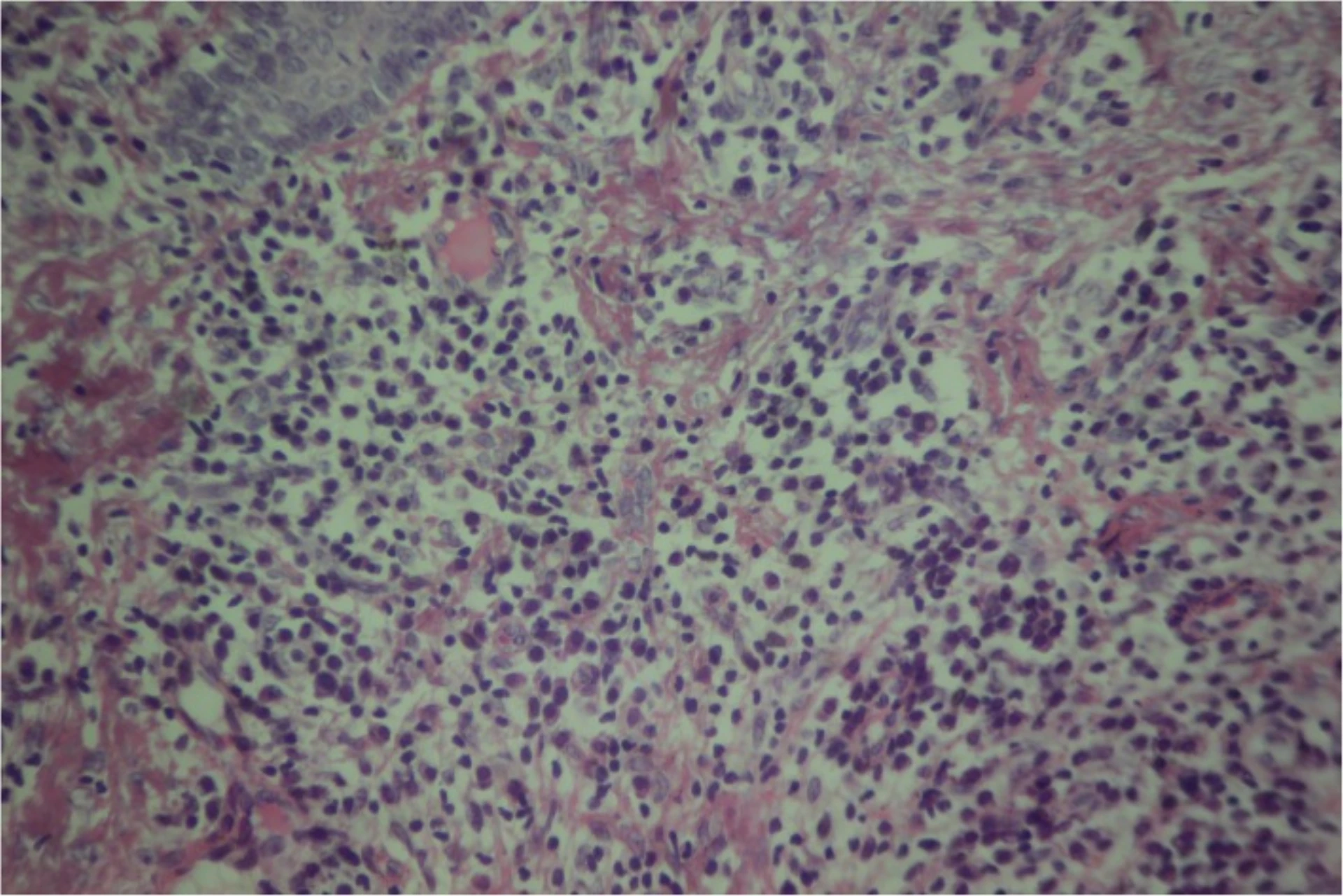
Study authors / courtesy of Dr. Camille Toledo, via Wikimedia · CC BY 4.0
Bleeding.
Most common. Manage with pressure, aluminum chloride 20%, or a single 4-0 / 5-0 nylon suture. Review anticoagulation status to prevent recurrence.
Infection.
< 1% with standard prep. Presents 48–72 h with erythema, warmth, drainage. Wound culture, empirical oral antibiotics covering MRSA + streptococci, escalate per Post-Test Q11.
Scarring & dyschromia.
Universal with punch. Counsel pre-procedure especially in Fitzpatrick IV–VI. Hyperpigmentation and keloid at chest / back are zone-specific risks.
Anesthetic hypersensitivity.
True lidocaine allergy rare; epinephrine-mediated vasovagal more common. Document history pre-procedure; have appropriate resuscitation accessible.
Non-diagnostic specimen.
Wrong site · crush artifact · inadequate depth · wrong fixative. Repeat biopsy if clinical suspicion persists — and review which gate was skipped.
Suspected melanoma.
Refer to dermatology for excisional. Punch risks understaging via sampling error — AAD position. Two rules collide on hands / face / feet: anatomic exclusion + melanoma rule.
Formalin instead of Zamboni for SFN.
The most common neurology-specific failure. Formalin destroys the IENF stain. Specimen is unsalvageable — patient is re-biopsied. Confirm fixative at the bedside before the punch leaves the room.
Wrong area biopsied.
Random or patient-preferred site instead of the most abnormal-appearing edge of an actively growing lesion (UCI Post-Test Q3) — or instead of the protocol-specified SFN / α-synuclein site. Site selection drives diagnostic yield.
Inadequate depth.
Surface-only punch misses panniculitis, deep vasculitis, the SFN dermal substrate, and synuclein deposits. Advance to the resistance change — full-thickness, every time. 2–3 mm rarely diagnostic for panniculitis; 6–8 mm reaches subcutis.
Missed melanoma rule.
Punch biopsy of a suspected pigmented melanocytic lesion understages via sampling error. Refer for excisional per AAD. On hands / face / feet two rules apply at once — anatomic exclusion AND the melanoma rule.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of punch-biopsy privilege | 5 independent cases per Master P&P §8.1 · mixed indications · within 6 months |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review on complication or repeat biopsy |
| Lapse | < 3 cases / rolling 24 mo | Skills Validation Checklist + 2 proctored cases rated Independent · FPPE restarts on next 5 |
| Renewal | Biennial · TJC MS.07.01.03 | OPPE indicators aggregate · Chair sign-off |
- Complication rate < 5% aggregate; 100% per-case review on any event
- Specimen adequacy ≥ 95% on first attempt
- Documentation completeness 100% — time-out, consent, site, size, anesthetic, fixative, follow-up plan
- Pathology follow-up loop closure 100%
- Skills checklist — all 19 elements Independent per Competence Assessment
- Post-test pass ≥ 80% per TJC HR.01.06.01
- 01Pickett H. Shave and punch biopsy for skin lesions. Am Fam Physician. 2011;84(9):995–1002. PMID 22046939.
- 02Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13(1):46–54. PMID 9462495.
- 03Katzberg HD, So Y, Brannagan T, et al. AANEM Small Fiber Neuropathy Task Force — diagnostic and screening laboratory tests in the assessment of patients with SFN: evidence-based review. Muscle Nerve. 2026;73(6):952–960. PMID 41670166.
- 04Doppler K, Ebert S, Üçeyler N, et al. Cutaneous neuropathy in Parkinson's disease: a window into brain pathology. Acta Neuropathol. 2014;128(1):99–109. PMID 24788821.
- 05Yaukey J, Kaur D. Management of small fiber neuropathy: a clinical perspective. Muscle Nerve. 2026;73(3):380–384. PMID 41367223.
- 06Waqar S, Khan H, Zulfiqar SK. Skin biopsy as a diagnostic tool for synucleinopathies: a review. Cureus. 2023;15(10):e47179. PMID 38022110.
- 07Lauria G, Hsieh ST, Johansson O, et al. EFNS / PNS guideline on the use of skin biopsy in the diagnosis of small-fiber neuropathy. Eur J Neurol. 2010;17(7):903–12.
- 08Kopp SL, Bateman BT, Cohen NH, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: ASRA-PM Evidence-Based Guidelines, 5th ed. Reg Anesth Pain Med. 2025. PMID 39880411.
- 09American Academy of Dermatology. Position statement and practice guideline — biopsy technique for suspected melanoma (full-thickness excisional preferred over punch).
- 10The Joint Commission. Universal Protocol UP.01.03.01 · HR.01.06.01 · MS.07.01.03 · MS.08.01.01 · MS.08.01.03. TJC Hospital Accreditation Standards; 2024.
- 11UCI APP Class II Master P&P §8.1 (5-case FPPE universal rule) · UCI APP Class 2 Training Plan Process, April 2026 · UCI canonical Punch Biopsy Competence Assessment (19 elements) · UCI canonical Punch Biopsy Post-Test.