Lumbar
Puncture.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 06_Lumbar_Puncture_Training_Plan.docx
- Suspected CNS infection — CSF closes the diagnosis; antibiotics not delayed for imaging.
- SAH workup when non-contrast head CT is negative — xanthochromia is the late-window signal.
- Idiopathic intracranial hypertension — opening-pressure manometry is the diagnosis.
- Demyelinating / inflammatory CNS workup — oligoclonal bands, IgG index, cytology.
- Intrathecal access — chemotherapy, antibiotics, anesthetic; dual-practitioner verification required.
Engelborghs S et al. Alzheimers Dement (Amst). 2017;8:111–126
Anatomy & landmarks.
Locate the conus terminus (~L1–L2), target L3–L4 or L4–L5; identify Tuffier's intercristal line at L4.
Indications & contras.
State accepted indications; apply Hasbun pre-LP CT rule; recite platelet, INR, and LMWH thresholds.
Atraumatic technique.
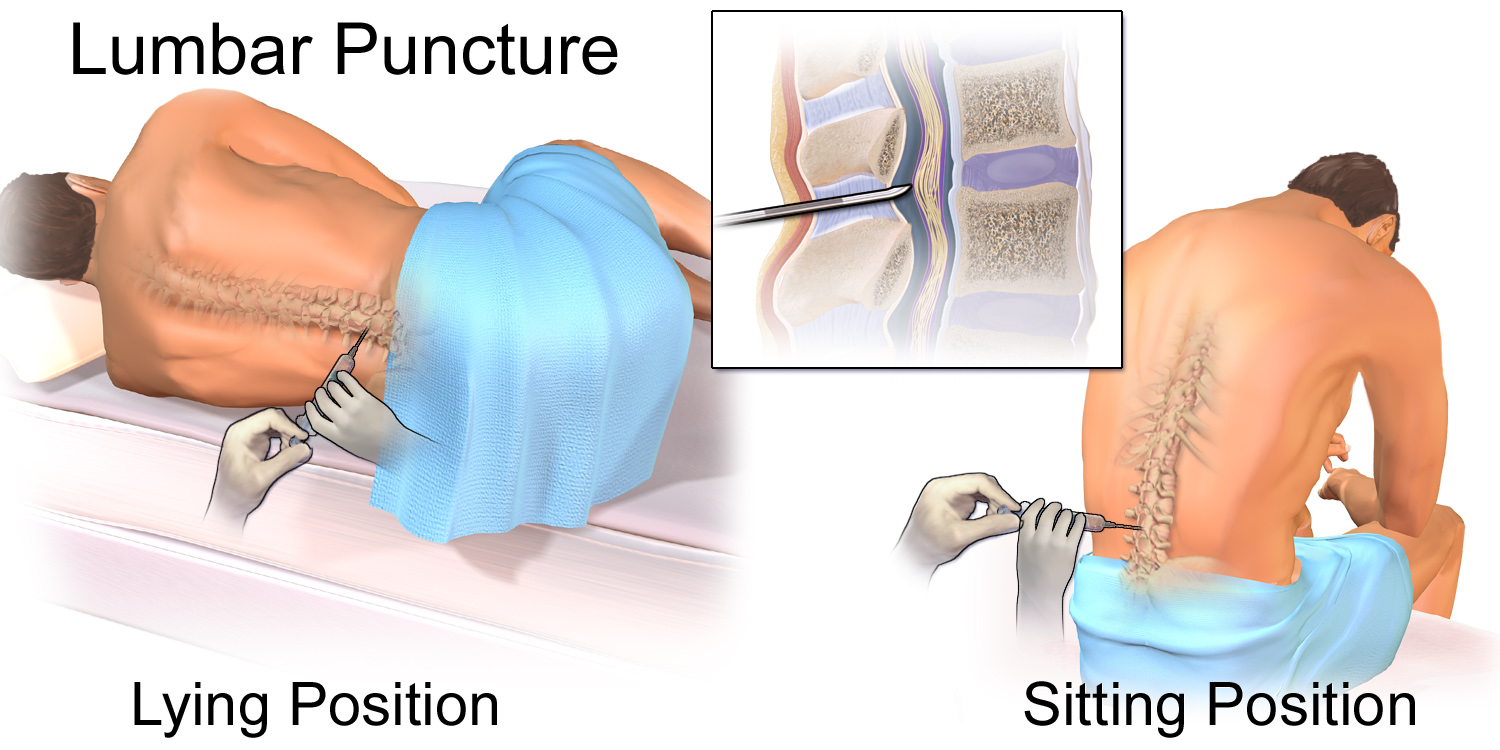
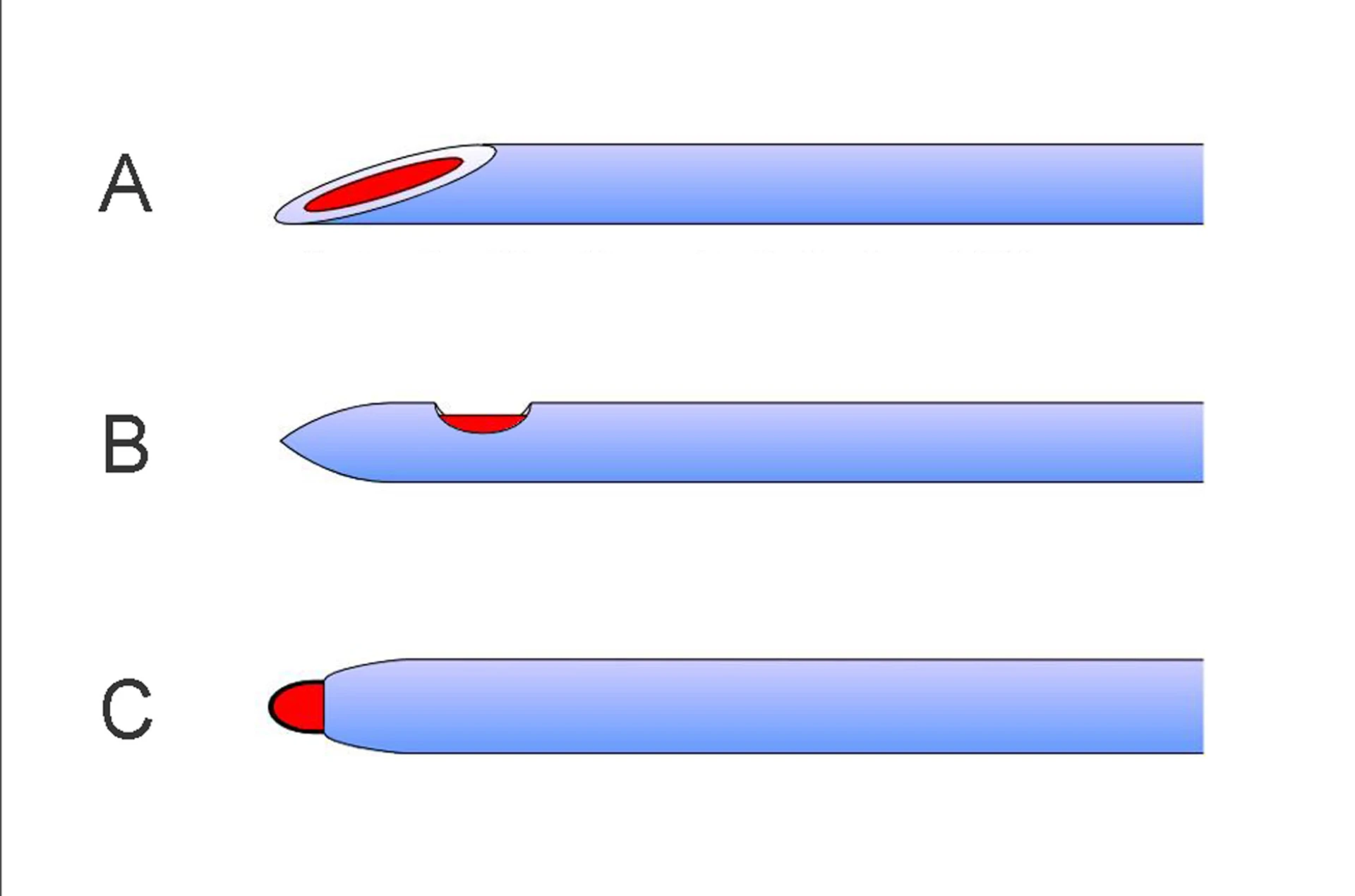
Position, prep, midline insertion with bevel parallel to dural fibers; stylet replaced before withdrawal.
Opening-pressure physics.
Connect manometer, measure in lateral decubitus with legs extended; recognize seated reading as invalid.
Four-tube sequence.
Collect tubes 1→4 with appropriate volumes; interpret tube-1 vs tube-4 RBC for traumatic-tap discrimination.
IT chemo verification.
Lead dual-practitioner verification of agent, dose, route; escalate complications per UCI policy.
- Conus medullaris terminates at approximately L1–L2 in adult anatomy.
- Target interspaces L3–L4 or L4–L5 — well below the conus.
- Cauda equina nerve roots float in CSF within the lumbar cistern — displaced by a midline needle.
- Dural sac extends to approximately S2; the subarachnoid space narrows below the cistern.
- Layered tissue planes encountered by the needle: skin → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space → dura.
Boon JM, Abrahams PH, Meiring JH, Welch T. Clin Anat. 2004;17(7):544–553
- Palpate the superior aspect of the posterior iliac crests bilaterally.
- Draw Tuffier's (intercristal) line between them — crosses at approximately the L4 spinous process or L4–L5 interspace.
- L3–L4 is one interspace cephalad to the line; L4–L5 sits at or just below it.
- PSIS, ASIS, and umbilicus are not the LP landmark (canonical post-test Q7).
- Interpatient variation exists vs MRI — confirm by palpating the spinous gap; consider ultrasound for difficult anatomy.
Suspected meningitis / encephalitis.
CSF cell count, Gram stain, culture, glucose, protein, viral PCR. Empiric antibiotics in parallel — never delayed for CT or LP per IDSA Tunkel 2017.
SAH with negative CT.
Beyond the early high-sensitivity CT window — xanthochromia by spectrophotometry at ≥12 h after symptom onset is the late-window CSF signal per Edlow 2000.
Opening-pressure manometry.
Idiopathic intracranial hypertension diagnosis (Friedman 2013); normal-pressure hydrocephalus workup; high-pressure headache evaluation.
Demyelinating / inflammatory CNS.
Oligoclonal bands, IgG index, paraneoplastic and autoimmune panels, cytology in suspected leptomeningeal disease.
Acute leukemia / high-grade lymphoma.
Cytology and flow cytometry for leptomeningeal involvement — per UCI canonical post-test Q1 indication list.
IT medication delivery.
Chemotherapy (methotrexate, cytarabine), intrathecal antibiotics, spinal anesthesia — dual-practitioner verification required.
- Clinical features of elevated ICP with mass effect without prior imaging clearance — see Hasbun rule, next slide.
- Severe uncorrected coagulopathy.
- Platelets < 40,000/µL for elective LP; < 20,000/µL for urgent LP with platelet transfusion support; absolute floor < 12,000/µL per spontaneous-bleed risk.
- Therapeutic-dose enoxaparin within 24 h (longer hold if renal impairment).
- Localized infection at the planned insertion site.
- Mild thrombocytopenia (50–100k) — case-by-case with hematology input.
- Antiplatelet therapy (aspirin, P2Y12 inhibitors) — usually proceed; document.
- DOAC therapy — hold per agent-specific protocol; consult pharmacy.
- Anatomic abnormality (severe scoliosis, prior fusion) — consider fluoroscopic guidance.
- Recent epidural anesthesia or known spinal pathology — escalate.
Head CT before LP
when Hasbun criteria fire.
- Altered mental status
- Focal neurologic deficit
- Papilledema on funduscopic exam
- Seizure within the prior week
- Age > 60
- Immunocompromised state
When meningitis is suspected, empiric coverage goes in as soon as blood cultures are drawn — imaging delay is not a reason to delay antibiotics. The LP itself is what waits on the CT.
Park N, Nigo M, Hasbun R. Comparison of four international guidelines on the utility of cranial imaging before LP in adults with bacterial meningitis. Clin Neuroradiol. 2022;32(3):857–862 · PMID 35181803
Tunkel AR et al. Clin Infect Dis. 2017;64(6):e34–e65 (IDSA)
- 01Consent documented. Indication, alternatives, material risks including post-LP headache, bleeding, infection, traumatic tap, and rare herniation. Surrogate engaged if patient lacks capacity.
- 02Labs reviewed. Platelets, INR, anticoagulation status. Enoxaparin held ≥ 24 h. DOACs per agent-specific protocol.
- 03Imaging decision made. Head CT first if any Hasbun criterion is present; document the decision in the procedure note.
- 04Positioning. Lateral decubitus with knees-to-chest and chin tuck when opening pressure is required; seated upright acceptable for landmark identification when OP is not measured.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, level when marked, equipment, consent confirmed aloud. For IT chemotherapy, add dual-practitioner agent / dose / route verification.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
22g preferred.
to dural fibers.
before withdrawal.
- Chlorhexidine-alcohol skin prep
- Sterile drape (fenestrated)
- Cap, mask, eye protection, sterile gown & gloves
- 1% lidocaine + 25g needle + 10 mL syringe
- Atraumatic spinal needle (22g preferred) — Whitacre / Sprotte
- Cutting Quincke needle as backup only
- Manometer with three-way stopcock
- Four numbered CSF collection tubes
- Gauze · sterile occlusive dressing
- Preservative-free saline for manometer priming (per institutional protocol)
Position ·
mark the interspace.
- Lateral decubitus, knees-to-chest, chin tucked
- Hips and shoulders perpendicular to the bed
- Mark L3–L4 or L4–L5 using Tuffier's line
- Seated alternative acceptable — but OP invalid in seated
Sterile prep ·
anesthesia.
- Chlorhexidine-alcohol, concentric circles, allow dry time
- Full barrier: cap, mask, eye protection, gown, gloves
- Sterile fenestrated drape
- Lidocaine 1% — wheal at entry, then deeper infiltration

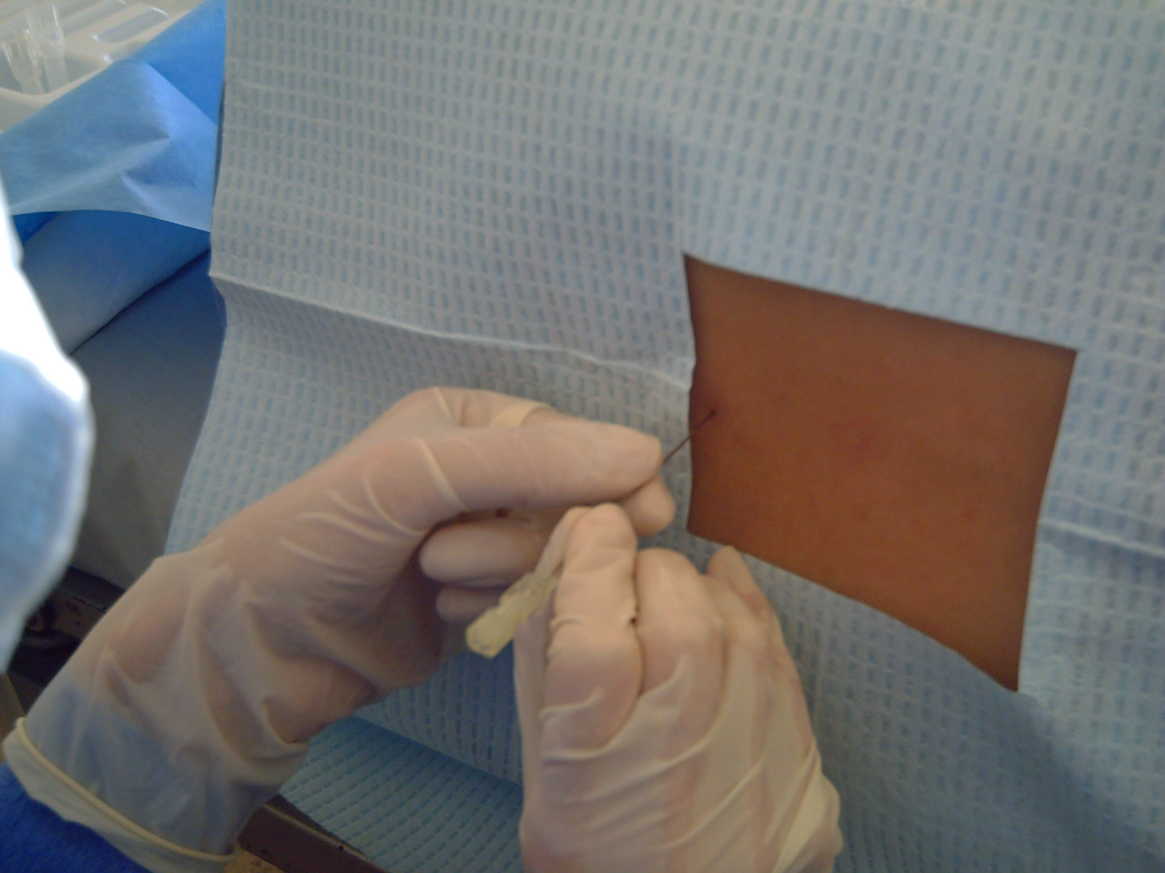
Needle in ·
midline, parallel.
- Atraumatic 22g, midline, ~15° cephalad
- Bevel parallel to long-axis dural fibers — splits, not cuts
- Advance through ligaments → ligamentum flavum → dura
- Withdraw stylet — clear CSF return is the definitive confirmation

Do not withdraw
halfway and reinsert.
- Reposition the patient — improves spinal flexion, opens the interspace.
- Rotate the needle 90° — clears a nerve root or arachnoid web off the bevel.
- Aspirate gently with a syringe — a few drops to break a low-flow column.
Withdrawing the needle halfway and re-advancing risks losing subarachnoid position and increases traumatic-tap rate on the next pass. Coughing is not a standard maneuver either.
- Lateral decubitus only — legs extended, patient relaxed, neutral spine.
- Connect manometer via three-way stopcock; read at the meniscus.
- Normal adult range: approximately 6–25 cm H2O.
- Seated reading is invalid — the hydrostatic CSF column above the puncture site artificially elevates the value (post-test Q8).
- ≥ 25 cm H2O with otherwise normal CSF → consider IIH per Friedman 2013.

Korsbæk JJ et al. Diagnosis of IIH: a proposal for evidence-based diagnostic criteria. Cephalalgia. 2023;43(3):3331024231152795 · PMID 36786317
| Tube | Test |
|---|---|
| 1 | Cell count + differential |
| 2 | Glucose, protein, chemistry |
| 3 | Gram stain + culture |
| 4 | Cell count + differential (vs tube 1) · reserved volume for cytology, OCBs, viral PCR |

- Replace the stylet before withdrawing the needle — reduces post-LP headache per Strupp 1998 (mechanism: prevents arachnoid fragment from being drawn through the dura).
- Withdraw the needle in a smooth, controlled motion.
- Apply gentle pressure with sterile gauze; place sterile occlusive dressing.
- Patient remains supine briefly; ambulate when comfortable.
- Post-procedure orders: oral hydration, analgesia, no requirement for prolonged bedrest — neither bedrest nor supplemental fluids prevent PDPH per Uppal 2024 multisociety consensus.
Uppal V et al. Evidence-based clinical practice guidelines on PDPH: a consensus report from a multisociety international working group. Reg Anesth Pain Med. 2024;49(7):471–501 · PMID 37582578
Post-LP headache.
Positional, worse upright. Conservative: hydration, analgesia, caffeine 300–500 mg PO. Blood patch if refractory beyond 48–72 h (post-test Q11).
Transient back pain.
Local soft-tissue trauma. Self-limited. NSAIDs or acetaminophen.
Traumatic tap.
Diagnostic ambiguity. Tube 1 vs Tube 4 RBC clearing argues against true SAH (post-test Q13).
Radicular pain.
Transient nerve-root irritation. Withdraw and redirect. Persistent radiculopathy → escalate.
Infection.
Meningitis or local site infection. Rare with chlorhexidine prep and sterile technique. Reportable event.
Epidural / spinal hematoma.
Coagulopathy or LMWH-bridged patients. Acute back pain + neurologic deficit = MRI + neurosurgery emergency.
Cerebellar herniation.
Elevated ICP with mass effect missed pre-LP. Prevention is the Hasbun rule — there is no rescue once herniation begins.
Diagnostic ambiguity.
Indeterminate CSF — repeat at a different interspace, image-guidance, or hematology / oncology consult.
- Independent dual-practitioner verification of patient, agent, dose, and route — per USP <800> and ONS Chemotherapy Standards (post-test Q14).
- Confirm CSF return at the spinal needle hub before injection.
- Remove an equivalent CSF volume before injecting the chemotherapy agent.
- Slow injection through the in-place spinal needle.
- 30-minute supine observation period post-injection; needle withdrawn after volume verified.
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of LP privilege | First 5 independent LPs · per-case review within 14 days · aggregate at 5 cases |
| OPPE | Continuous baseline | Every 6 mo · 10% sample (min 2, max 10) · 100% review on severe complication |
| Lapse | < 3 LPs in 24 mo | Stream C simulation + 2 proctored cases before independent practice resumes |
- First-attempt success ≥ 80%
- Atraumatic-needle utilization ≥ 95%
- Traumatic-tap rate < 10% · post-LP headache rate < 10%
- Pre-LP CT use when Hasbun-indicated ≥ 95%
- Severe complication review 100%
- 01Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before lumbar puncture in adults with suspected meningitis. N Engl J Med. 2001;345(24):1727–1733.
- 02Engelborghs S et al. Consensus guidelines for lumbar puncture in patients with neurological diseases. Alzheimers Dement (Amst). 2017;8:111–126.
- 03Tunkel AR et al. The IDSA's clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. 2017;64(6):e34–e65.
- 04Boon JM, Abrahams PH, Meiring JH, Welch T. Lumbar puncture: anatomical review of a clinical skill. Clin Anat. 2004;17(7):544–553.
- 05Standring S, ed. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Elsevier; 2021.
- 06Arendt K, Demaerschalk BM, Wingerchuk DM, Camann W. Atraumatic lumbar puncture needles: after all these years, are we still missing the point? Neurologist. 2009;15(1):17–20.
- 07Strupp M, Brandt T, Müller A. Incidence of post-lumbar puncture syndrome reduced by reinserting the stylet. J Neurol. 1998;245(9):589–592.
- 08Uppal V, Russell R, Sondekoppam RV, et al. Evidence-based clinical practice guidelines on postdural puncture headache: a consensus report from a multisociety international working group. Reg Anesth Pain Med. 2024;49(7):471–501. PMID 37582578.
- 09Friedman DI et al. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013;81(13):1159–1165.
- 10Korsbæk JJ, Jensen RH, Høgedal L, et al. Diagnosis of idiopathic intracranial hypertension: a proposal for evidence-based diagnostic criteria. Cephalalgia. 2023;43(3):3331024231152795. PMID 36786317.
- 11Edlow JA, Caplan LR. Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. N Engl J Med. 2000;342(1):29–36.
- 12Mayeaux EJ Jr. Essential Guide to Primary Care Procedures. 2nd ed. Wolters Kluwer; 2015.
- 13Kopp SL, Vandermeulen E, McBane RD, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: ASRA-PM evidence-based guidelines (5th ed). Reg Anesth Pain Med. 2025. PMID 39880411.
- 14Park N, Nigo M, Hasbun R. Comparison of four international guidelines on the utility of cranial imaging before LP in adults with bacterial meningitis. Clin Neuroradiol. 2022;32(3):857–862. PMID 35181803.
- 15The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 16UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. May 2026.