Laceration
Repair.
APP Education · Department of Neurology
Approving authority: Claire Henchcliffe, MD, DPhil · Chair, Department of Neurology
Source-of-truth: 01_Procedures/15_Laceration_Repair/
- Highest-volume bedside procedure across the APP service — every shift, every site.
- The technique is simple; the decision architecture around it is not — wound assessment drives every downstream choice.
- Two preventable failure modes dominate malpractice exposure: missed deeper injury (tendon, nerve, foreign body) and local anesthetic systemic toxicity.
- UCI OPPE target: documented infection < 3%, dehiscence < 2%, cosmetic revision < 2%.
StatPearls — Wound Closure Techniques · NCBI Bookshelf NBK470598
Position the patient.
Ergonomic operator access and adequate lighting — the UCI canonical step says "make it comfortable for you the provider."
Indication, contra, complication.
State indications for primary closure; recite the verbatim UCI contraindication list; recognize the four canonical complications.
Anesthesia ceilings.
Calculate lidocaine max — 4.5 mg/kg plain, 7 mg/kg with epi — and identify the five epi-forbidden distal-appendage sites.
Irrigation & sterile field.
1–2 L normal saline, moderate pressure, 50–100 mL per cm of wound. CHG prep, sterile drape, sterile gloves.
Closure-method choice.
Sutures vs staples vs tissue adhesive — matched to location, length, tension, contamination. Simple interrupted is the workhorse.
LAST recognition.
Verbalize epi-forbidden sites pre-injection; recognize LAST prodrome (perioral numbness, tinnitus, metallic taste) and activate ASRA protocol.
Sharp · crush · bite · glass.
Drives contamination risk and the question of whether to close at all. Bite mechanism is typically not closed primarily.
Golden-period window.
Simple < 5 cm, no gross contamination, non-LE — closable up to 12–18 h per Forsch 2017. Face shorter; LE shorter.
Clean · contaminated · gross.
If you can't irrigate it clean, you can't close it primarily. Heavily contaminated → delayed primary or secondary intention.
Face · scalp · trunk · limb.
Determines closure window, suture size, removal timing, cosmetic stakes, and which closure method is appropriate.
Epidermis · dermis · fat · fascia.
Deeper than mid-dermis needs layered closure (absorbable dermal + non-absorbable skin). Through fascia escalates.
Tendon · nerve · vessel · foreign body.
Always do a distal neurovascular exam — sensation, motor, capillary refill, pulse. Exposed deep structure → do not close, escalate.
| Closure type | Indication | Window | Why |
|---|---|---|---|
| Primary intention | Clean simple laceration · edges approximate · no gross contamination | Face ≤ 6 h · trunk ≤ 12 h · scalp ≤ 24 h · simple < 5 cm non-LE ≤ 12–18 h | Best cosmetic result, fastest healing, lowest re-visit rate. |
| Delayed primary | Grossly contaminated · cannot irrigate clean today | Pack open · re-evaluate at 72–96 h | Allow inflammatory phase to declare, then close if bed is clean. |
| Secondary intention | High bacterial load · tissue loss · edges will not approximate | — | Let it close on its own — scar is worse, infection risk is lower. |
| Tissue adhesive | Low-tension · short · clean · off the face if cosmetic stakes high | Within standard golden period | Painless, fast, no removal — but not for high-tension or hair-bearing scalp. |
| Staples | Scalp · trunk · extremity (not face, not hand) | Within standard golden period | Fast, hemostatic, low infection rate; cosmetic match for scalp. |
- Bite wounds — animal & human
- Grossly contaminated wounds
- Tissue loss — edges will not approximate
- Involvement of underlying structures
- Complex facial or hand wounds
- Chronic wounds
- Cat bite to the hand → infection risk dominates; do not close · cover with augmentin · escalate
- Human bite to the hand (clenched-fist injury) → emergent hand surgery, not a bedside closure
- Exposed tendon, nerve, vessel, joint capsule, bone → escalate to hand surgery, plastics, or ED attending
- Heavily contaminated wound past the golden period → delayed primary or secondary intention
- Devitalized tissue requiring formal debridement → operating-room debridement, not bedside
- Wound under arterial tension that will not approximate → flap repair, not simple closure
- Perioral numbness · metallic taste
- Tinnitus · diplopia · agitation
- Late: seizure · cardiac arrest
- 1% lidocaine (± epi 1:100,000)
- 25g needle for infiltration · 27g for face
- 10–20 mL syringe for anesthetic
- 30–60 mL syringe + 18g angiocath / splash shield
- 1–2 L normal saline (irrigation)
- CHG-alcohol prep
- Sterile gloves · sterile drape · gauze
- Needle driver · Adson forceps · iris scissors
- Suture by location (size + material)
- Stapler (scalp) · tissue adhesive (low-tension small)
- Xeroform + sterile gauze for dressing
- Tetanus (Td or TdAP) per ACIP if indicated
- Hemostat · vessel ligature (if bleeding)
- Calculate lidocaine max by weight — verbalize during time-out
- Choose plain vs epi — verbalize epi-forbidden sites aloud
- Inject through wound edges (less painful than through skin)
- Slow injection · aspirate before each bolus
- Wait 5–10 min for full onset (UCI canonical timing)
- Test for adequate anesthesia before any cutting
- Cumulative-dose discipline — track every mL given
- 01Consent documented. Indication, risks (infection, pain, neurovascular injury, scar, LAST), alternatives (delayed primary, referral, secondary intention), right to decline. Cosmetic-outcome discussion mandatory for face/scalp.
- 02Allergies & tetanus reconciled. Lidocaine / amide allergy? Latex? Adhesive? Tetanus status per CDC ACIP — Td or TdAP indicated?
- 03Lidocaine dose calculated. Weight-based max — verbalize the calculation aloud. Decide plain vs epinephrine.
- 04Epi-forbidden sites verbalized. Fingers · Toes · Ears · Nose · Penis — audible safety pause if epi is on the tray.
- 05Time-out called. Per TJC UP.01.03.01 — correct patient, procedure, site / side, equipment, consent confirmed aloud.
UP.01.03.01
TJC Hospital Accreditation Standards · 2024.
Position ·
provider comfort.
- Patient supine or seated, wound visible
- Adjust bed / chair height to your hands
- Adequate lighting · headlamp if needed
- "Make it comfortable for you the provider"
Irrigate ·
1–2 L saline.
- 50–100 mL per cm of wound length
- Moderate pressure (5–8 PSI)
- 30–60 mL syringe + 18g angiocath / splash shield
- Tap water = saline for simple wounds (Cochrane)
Prep ·
sterile field.
- CHG-alcohol skin prep · allow to dry
- Sterile gloves · sterile drape
- Open suture tray on sterile field
- Drape head-to-toe-of-wound, not just the cut
Anesthetize ·
wait 5–10 min.
- Inject through wound edges, slow
- Aspirate before each bolus
- Track cumulative mL against weight-based max
- Wait 5–10 min then test before cutting
- Inspect the base under anesthesia — tendon, nerve, vessel, foreign body
- Foreign body found → remove if shallow, image if retained
- Devitalized tissue → judicious debridement, sharp, conservative
- Hemostasis — direct pressure, hemostat, vessel ligation if needed
- Exposed deep structure → STOP, escalate, do not close
- Simple interrupted — workhorse for most acute lacerations
- Eversion · equal bites · depth equal to width · knot off to the side
- Tension-free apposition — if it pulls, change the plan
- Layered closure if deep — absorbable dermal + non-absorbable skin
- Technique geometry taught in Procedure 08 — Suturing
| Method | Best for |
|---|---|
| Sutures | Most lacerations · cosmetic stakes · high-tension areas |
| Staples | Scalp · trunk · extremity (fast · hemostatic) |
| Adhesive | Short · low-tension · clean · cooperative patient |
Staples first.
Fast, hemostatic, cosmetically acceptable under hair. Alternative: 3-0 or 4-0 nylon. Remove at 7–10 days.
Align the border.
First stitch goes through the vermillion border — exact alignment matters more than anything else on the face. 1 mm off is visible at 6 months.
Cover the cartilage.
Close perichondrium first, then skin. Never leave cartilage exposed under skin — chondritis risk.
No epi · refer if nailbed.
Plain lidocaine only (epi-forbidden). Nailbed laceration → repair with absorbable 6-0; consider hand-surgery consult.
Do not close.
Cat & human bites to the hand → infection risk dominates. Augmentin, escalation, often no primary closure.
Escalate.
Stellate, flap, avulsion — geometric closure outside bedside-APP scope. Plastics or ED attending.
Check NV exam.
Sensation, motor, capillary refill, pulse — every laceration with extremity depth gets a documented exam before closure.
Sedation question.
If cooperation insufficient and wound is non-trivial → escalate for ED procedural sedation, not bedside force.
Stop injecting.
Stop closing.
Perioral numbness, tinnitus, metallic taste, diplopia — any one means stop the injection, ABCs, call for help. Severe: 20% lipid emulsion 1.5 mL/kg lean body mass bolus, then infusion. Per ASRA LAST 2020.
Exposed tendon, nerve, vessel, joint capsule, bone — or any positive neurovascular finding distal to the wound — do not close. Pack moist gauze, dressing, escalate to hand surgery or plastics.
injury is the malpractice case.
Reg Anesth Pain Med. 2021;46(1):81–82
| Event | Rate | Mitigation |
|---|---|---|
| Wound infection | 1–5% | Irrigation volume · stewardship · close past golden period only when safe |
| Dehiscence | < 2% | Tension-free closure · appropriate suture size/material · accurate removal timing |
| Hypertrophic / keloid scar | variable | Patient counseling · sun protection · silicone gel · dermatology referral |
| Missed deeper injury | — | Mandatory NV exam · base inspection under anesthesia · escalate if uncertain |
| Foreign body retention | — | Direct inspection · imaging if suspected radiopaque material |
| Allergic reaction | rare | True amide allergy uncommon · preservative more often culprit · preservative-free vial |
| LAST | rare · catastrophic | Weight-based dose calc · cumulative tracking · ASRA 2020 protocol |
- Skipping tetanus reconciliation. Every traumatic laceration gets a tetanus status check; Td or TdAP per CDC ACIP if non-current.
- Inadequate irrigation. Tablespoons, not liters. 50–100 mL per cm of wound or you are guaranteeing infection.
- Closing past the golden period on a contaminated wound — delayed primary or secondary intention.
- Cumulative lidocaine error. "Just a little more" stacks. Track every mL, calculate the ceiling before you start.
- Missing the deep injury. No NV exam, no base inspection — closure over a transected tendon ends in court.
StatPearls Wound Closure · NBK470598 · CDC ACIP · tetanus prophylaxis
- Keep dressing dry for 24 hours; then gentle washing OK
- Watch for infection: spreading redness, increasing pain, fever, drainage
- Return precautions: opened wound, numbness/weakness distal, fever, drainage
- Scar care: sun protection · silicone gel once closed · expect 6–12 mo to mature
- Tetanus: Td or TdAP per CDC ACIP if non-current — administered or scheduled
- Antibiotic stewardship: not for clean wounds; indicated for bites, puncture, immunocompromised
- Document every instruction given
| Location | Days |
|---|---|
| Face | 4–5 |
| Scalp | 7–10 |
| Trunk | 7–10 |
| Upper extremity | 7–10 |
| Lower extremity | 10–14 |
| Joint-crossing | 10–14 · immobilize |
| Stage | Trigger | Scope |
|---|---|---|
| FPPE | Board approval of laceration-repair privilege | First 5 independent cases · per-case review < 14 days · aggregate at 5 |
| Case mix | FPPE pass criterion | ≥ 1 face/scalp · ≥ 1 extremity · ≥ 1 with debridement |
| OPPE | Every 6 months (TJC MS.08.01.03) | 10% sample (min 2, max 10) · 100% review on complication / return / revision |
| Reinstatement | < 5 cases over 24 mo | Bench validation + 2 proctored cases · case mix preserved |
- Wound infection rate < 3%
- Dehiscence rate < 2%
- Return-visit for complication < 5%
- Cosmetic-revision request rate < 2%
- Documentation completeness 100%
- Tetanus reconciliation (indicated cases) 100%
- Antibiotic stewardship appropriate 100%
- Successful primary closure first attempt ≥ 95%
- 01Forsch RT, Little SH, Williams C. Laceration repair: a practical approach. Am Fam Physician. 2017;95(10):628–636.
- 02StatPearls — Wound Closure Techniques. National Center for Biotechnology Information, NCBI Bookshelf NBK470598.
- 03Neal JM, Neal EJ, Weinberg GL. ASRA Local Anesthetic Systemic Toxicity Checklist: 2020 version. Reg Anesth Pain Med. 2021;46(1):81–82.
- 04Nicks BA, Ayello EA, Woo K, Nitzki-George D, Sibbald RG. Acute wound management: revisiting the approach to assessment, irrigation, and closure considerations. Int J Emerg Med. 2010;3(4):399–407. PMC3047833.
- 05Fernandez R, Green HL, Griffiths R, Atkinson RA, Ellwood LJ. Water for wound cleansing. Cochrane Database Syst Rev. 2022;9(9):CD003861. doi:10.1002/14651858.CD003861.pub4.
- 06Centers for Disease Control and Prevention (CDC). ACIP Recommendations · Tetanus prophylaxis in wound management. CDC; current edition.
- 07The Joint Commission. Universal Protocol UP.01.03.01. TJC Hospital Accreditation Standards; 2024.
- 08The Joint Commission. HR.01.06.01 · MS.08.01.01 · MS.08.01.03 — competency & FPPE/OPPE. 2024.
- 09Mayeaux EJ. The Essential Guide to Primary Care Procedures. 2nd ed. Wolters Kluwer; 2015.
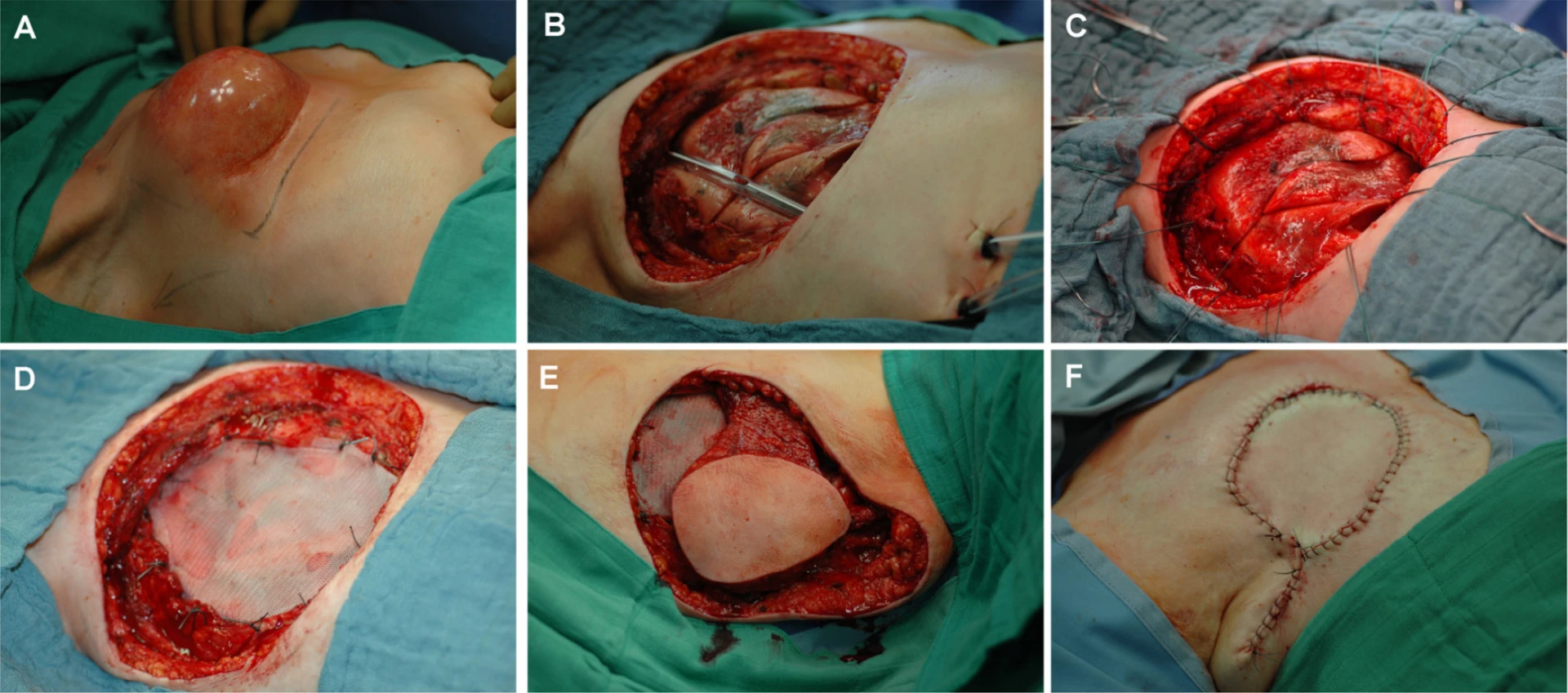
- 10Gerullis H, Heuck CJ, Schneider P. Layered wound closure following resection of radionecrosis (image). Wikimedia Commons · CC BY 2.0.
- 11UCI APP Class 2 Training Plan Process. Department of Neurology, University of California, Irvine. April 2026.
- 12UCI Neurology Laceration Repair Training Plan & Competence Assessment (canonical source documents). UCI Department of Neurology APP Education; 2026-05-05.